

Ulcerative colitis
- PMID: 27914657
- PMCID: PMC6487890
- DOI: 10.1016/S0140-6736(16)32126-2
Ulcerative colitis
Abstract
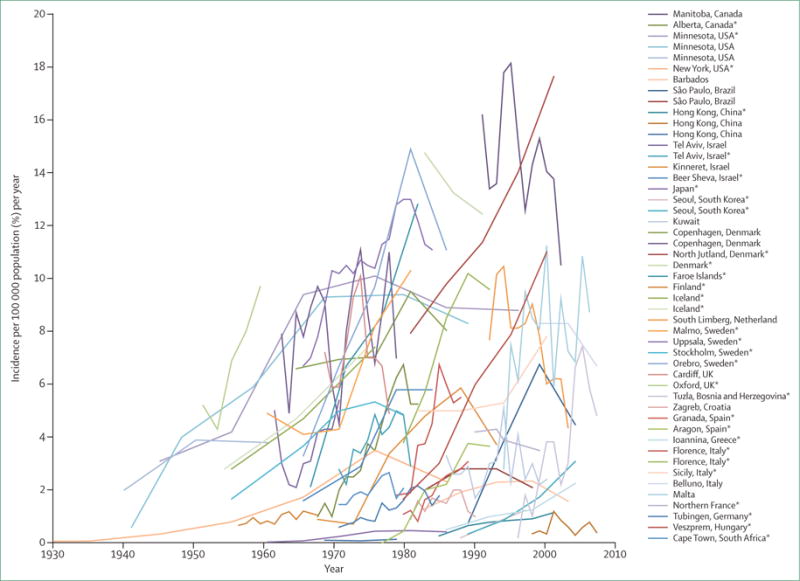
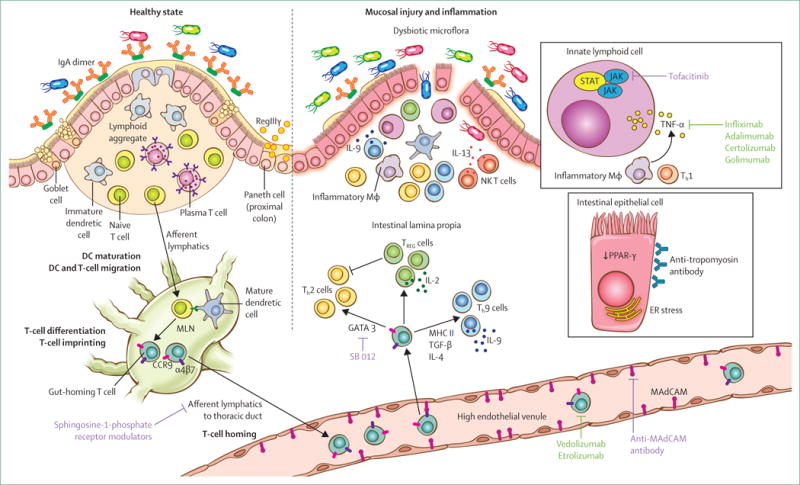
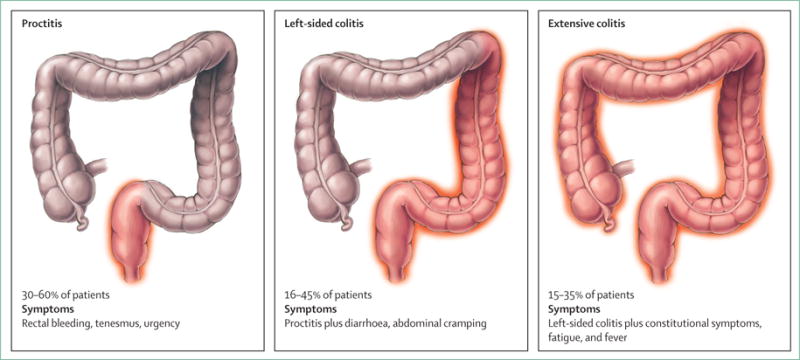
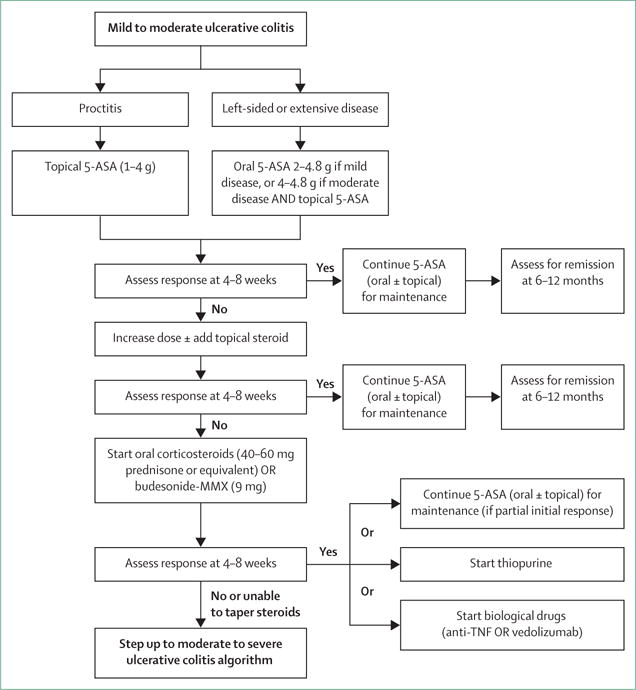
Ulcerative colitis is a chronic inflammatory disease affecting the colon, and its incidence is rising worldwide. The pathogenesis is multifactorial, involving genetic predisposition, epithelial barrier defects, dysregulated immune responses, and environmental factors. Patients with ulcerative colitis have mucosal inflammation starting in the rectum that can extend continuously to proximal segments of the colon. Ulcerative colitis usually presents with bloody diarrhoea and is diagnosed by colonoscopy and histological findings. The aim of management is to induce and then maintain remission, defined as resolution of symptoms and endoscopic healing. Treatments for ulcerative colitis include 5-aminosalicylic acid drugs, steroids, and immunosuppressants. Some patients can require colectomy for medically refractory disease or to treat colonic neoplasia. The therapeutic armamentarium for ulcerative colitis is expanding, and the number of drugs with new targets will rapidly increase in coming years.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
RCU has no conflicts of interest. SM has served as a consultant for Pfizer Inc and receives research funding support from Takeda Pharmaceuticals. PBA has received Speaker fees for MSD, AbbVie, Allergen, Ferring, Warner Chilcott, and Napp. LP-B has received consulting fees from Merck, AbbVie, Janssen, Genentech, Mitsubishi, Ferring, Norgine, Tillots, Vifor, Therakos, Pharmacosmos, Pilège, Bristol-Myers Squibb, Union Chimique Belge (UCB) Pharmaceuticals, Hospira, Celltrion, Takeda, Biogaran, Boerhinger-Ingelheim, Lilly, Pfizer, HAC Pharma, Index Pharmaceuticals, Amgen, Sandoz, Forward Pharma GmbH, Celgene, Biogen, Lycera, and Samsung Bioepis, and lecture fees from Merck, AbbVie, Takeda, Janssen, Takeda, Ferring, Norgine, Tillots, Vifor, Therakos, Mitsubishi, and HAC Pharma. J-FC has served as consultant or advisory board member for AbbVie, Amgen, AstraZeneca, ABScience, Boehringer, Bristol-Meyers Squibb, Celgene, Celltrion, Danone, Enterome, Evidera, Ferring, Genentech, Giuliani SPA, Given Imaging, Janssen & Janssen, Immune Pharmaceuticals, Intestinal Biotech Development, Kyowa Kirin Pharma, Lilly, Medimmune, Merck Sharp Dohme, Merck & Co, Millennium Pharmaceuticals Inc, Navigant Consulting, Neovacs, Nestle Nutrition Sciences Partner, Nutrition Science Partners Ltd, Pfizer, Prometheus Laboratories, Protagonist Therapies, Receptos, Sanofi, Schering Plough Corporation, Second Genome, Shire, Takeda, Teva Pharmaceuticals, Tigenix, UCB, UEGW AbbVie Advisory Board, UEGW AbbVie Symposium, Vertex, and Dr August Wolff GmbH Co.
Figures
References
-
- Høivik ML, Moum B, Solberg IC, et al. Work disability in inflammatory bowel disease patients 10 years after disease onset: results from the IBSEN Study. Gut. 2013;62:368–75. - PubMed
-
- Torres J, Billioud V, Sachar DB, Peyrin-Biroulet L, Colombel J-F. Ulcerative colitis as a progressive disease: the forgotten evidence. Inflamm Bowel Dis. 2012;18:1356–63. - PubMed
-
- Peyrin-Biroulet L, Sandborn W, Sands BE, et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): determining therapeutic goals for treat-to-target. Am J Gastroenterol. 2015;110:1324–38. - PubMed
-
- Magro F, Rodrigues A, Vieira AI, et al. Review of the disease course among adult ulcerative colitis population-based longitudinal cohorts. Inflamm Bowel Dis. 2012;18:573–83. - PubMed
-
- Cohen RD, Yu AP, Wu EQ, Xie J, Mulani PM, Chao J. Systematic review: the costs of ulcerative colitis in Western countries. Aliment Pharmacol Ther. 2010;31:693–707. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
