

Cognitive behavioural therapy and short-term psychoanalytical psychotherapy versus a brief psychosocial intervention in adolescents with unipolar major depressive disorder (IMPACT): a multicentre, pragmatic, observer-blind, randomised controlled superiority trial
- PMID: 27914903
- PMCID: PMC5285447
- DOI: 10.1016/S2215-0366(16)30378-9
Cognitive behavioural therapy and short-term psychoanalytical psychotherapy versus a brief psychosocial intervention in adolescents with unipolar major depressive disorder (IMPACT): a multicentre, pragmatic, observer-blind, randomised controlled superiority trial
Erratum in
-
Correction: Cognitive behavioural therapy and short-term psychoanalytical psychotherapy versus a brief psychosocial intervention in adolescents with unipolar major depressive disorder (IMPACT): a multicenter, pragmatic, observer-blind, randomized controlled superiority trial.Lancet Psychiatry. 2017 Aug;4(8):582. doi: 10.1016/S2215-0366(17)30283-3. Lancet Psychiatry. 2017. PMID: 28748793 Free PMC article. No abstract available.
Abstract
Background: Psychological treatments for adolescents with unipolar major depressive disorder are associated with diagnostic remission within 28 weeks in 65-70% of patients. We aimed to assess the medium-term effects and costs of psychological therapies on maintenance of reduced depression symptoms 12 months after treatment.
Methods: We did this multicentre, pragmatic, observer-blind, randomised controlled superiority trial (IMPACT) at 15 National Health Service child and adolescent mental health service (CAMHS) clinics in three regions in England. Adolescent patients (aged 11-17 years) with a diagnosis of DSM IV major depressive disorder were randomly assigned (1:1:1), via a web-based randomisation service, to receive cognitive behavioural therapy (CBT) or short-term psychoanalytical therapy versus a reference brief psychological intervention. Randomisation was stochastically minimised by age, sex, self-reported depression sum score, and region. Patients and clinicians were aware of group allocation, but allocation was concealed from outcome assessors. Patients were followed up and reassessed at weeks 6, 12, 36, 52, and 86 post-randomisation. The primary outcome was self-reported depression symptoms at weeks 36, 52, and 86, as measured with the self-reported Mood and Feelings Questionnaire (MFQ). Because our aim was to compare the two psychological therapies with the brief psychosocial intervention, we first established whether CBT was inferior to short-term psychoanalytical psychotherapy for the same outcome. Primary analysis was by intention to treat. This trial is registered with Current Controlled Trials, number ISRCTN83033550.
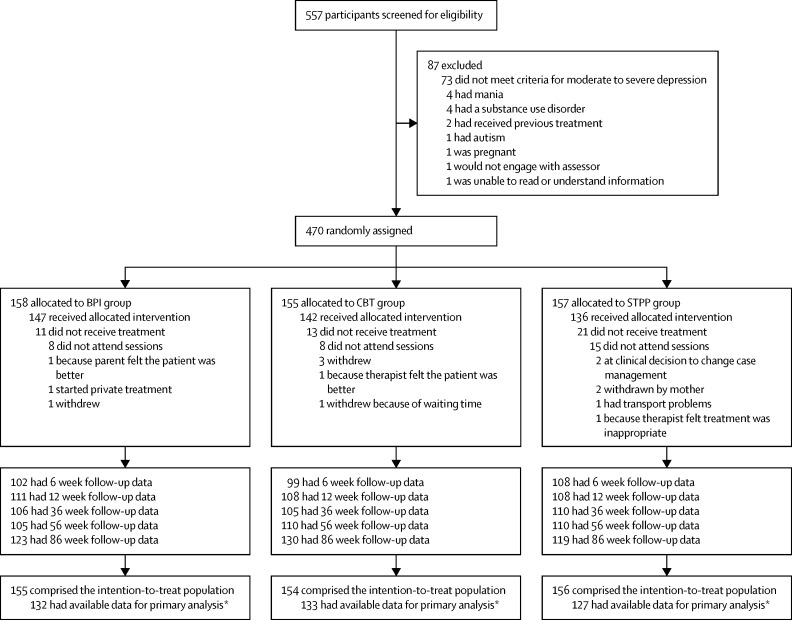
Findings: Between June 29, 2010, and Jan 17, 2013, we randomly assigned 470 patients to receive the brief psychosocial intervention (n=158), CBT (n=155), or short-term psychoanalytical therapy (n=157); 465 patients comprised the intention-to-treat population. 392 (84%) patients had available data for primary analysis by the end of follow-up. Treatment fidelity and differentiation were established between the three interventions. The median number of treatment sessions differed significantly between patients in the brief psychosocial intervention group (n=6 [IQR 4-11]), CBT group (n=9 [5-14]), and short-term psychoanalytical therapy group (n=11 [5-23]; p<0·0001), but there was no difference between groups in the average duration of treatment (27·5 [SD 21·5], 24·9 [17·7], 27·9 [16·8] weeks, respectively; Kruskal-Wallis p=0·238). Self-reported depression symptoms did not differ significantly between patients given CBT and those given short-term psychoanalytical therapy at weeks 36 (treatment effect 0·179, 95% CI -3·731 to 4·088; p=0·929), 52 (0·307, -3·161 to 3·774; p=0·862), or 86 (0·578, -2·948 to 4·104; p=0·748). These two psychological treatments had no superiority effect compared with brief psychosocial intervention at weeks 36 (treatment effect -3·234, 95% CI -6·611 to 0·143; p=0·061), 52 (-2·806, -5·790 to 0·177; p=0·065), or 86 (-1·898, -4·922 to 1·126; p=0·219). Physical adverse events (self-reported breathing problems, sleep disturbances, drowsiness or tiredness, nausea, sweating, and being restless or overactive) did not differ between the groups. Total costs of the trial interventions did not differ significantly between treatment groups.
Interpretation: We found no evidence for the superiority of CBT or short-term psychoanalytical therapy compared with a brief psychosocial intervention in maintenance of reduced depression symptoms 12 months after treatment. Short-term psychoanalytical therapy was as effective as CBT and, together with brief psychosocial intervention, offers additional patient choice for psychological therapy, alongside CBT, for adolescents with moderate to severe depression who are attending routine specialist CAMHS clinics.
Funding: National Institute for Health Research (NIHR) Health Technology Assessment (HTA) programme, and the Department of Health.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
From efficacy to pragmatic trials: does the dodo bird verdict apply?Lancet Psychiatry. 2017 Feb;4(2):84-85. doi: 10.1016/S2215-0366(16)30404-7. Epub 2016 Dec 1. Lancet Psychiatry. 2017. PMID: 27914904 No abstract available.
-
Hunting down an evidence base for adolescent mental health.Lancet Psychiatry. 2017 Feb;4(2):83. doi: 10.1016/S2215-0366(16)30443-6. Epub 2017 Jan 12. Lancet Psychiatry. 2017. PMID: 28089312 No abstract available.
-
The IMPACT trial - Authors' reply.Lancet Psychiatry. 2017 Apr;4(4):275-276. doi: 10.1016/S2215-0366(17)30086-X. Lancet Psychiatry. 2017. PMID: 28347429 No abstract available.
-
The IMPACT trial.Lancet Psychiatry. 2017 Apr;4(4):275. doi: 10.1016/S2215-0366(17)30087-1. Lancet Psychiatry. 2017. PMID: 28347430 No abstract available.
References
-
- Whiteford HA, Degenhardt L, Rehm J. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382:1575–1586. - PubMed
-
- March J, Silva S, Petrycki S. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial. JAMA. 2004;292:807–820. - PubMed
-
- Rush AJ, Wisniewski SR, Zisook S. Is prior course of illness relevant to acute or longer-term outcomes in depressed out-patients? A STAR*D report. Psychol Med. 2012;42:1131–1149. - PubMed
-
- National Institute for Health and Care Excellence . CG28: depression in children and young people: identification and management in primary, community and secondary care. National Institute for Health and Care Excellence; London: 2005.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
