

Effects of zacopride, a moderate IK1 channel agonist, on triggered arrhythmia and contractility in human ventricular myocardium
- PMID: 27914945
- PMCID: PMC5234043
- DOI: 10.1016/j.phrs.2016.11.033
Effects of zacopride, a moderate IK1 channel agonist, on triggered arrhythmia and contractility in human ventricular myocardium
Abstract
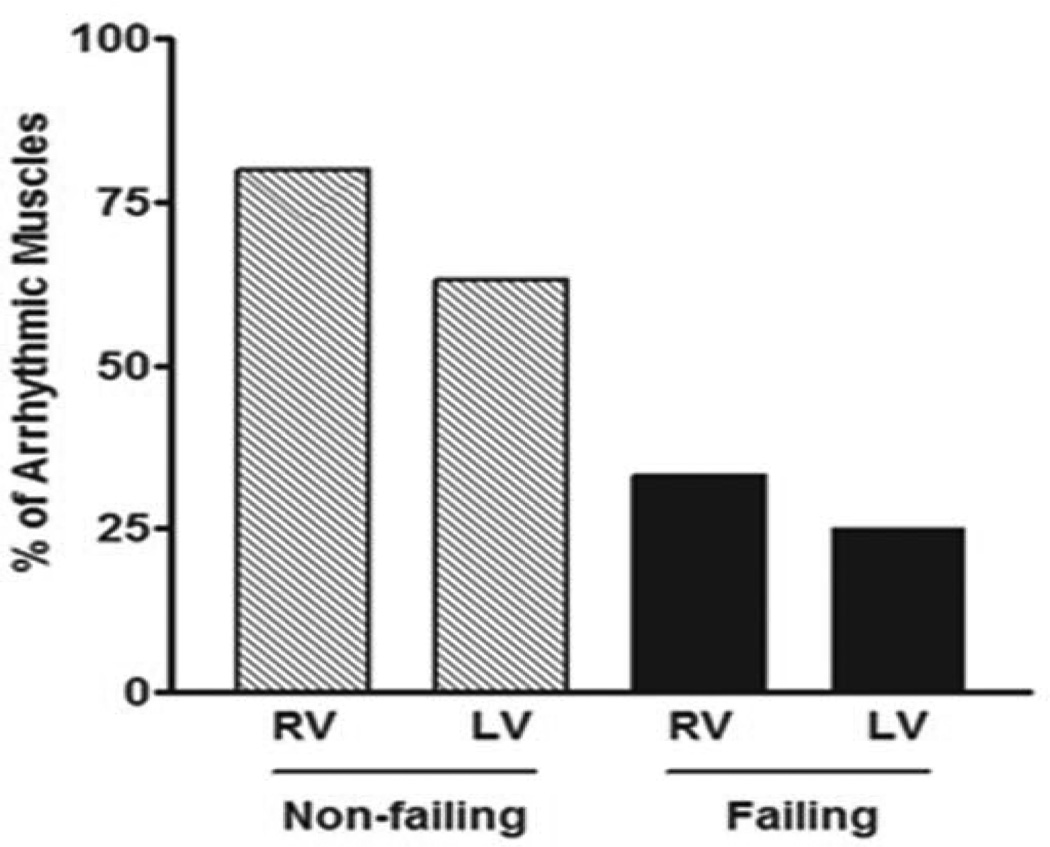
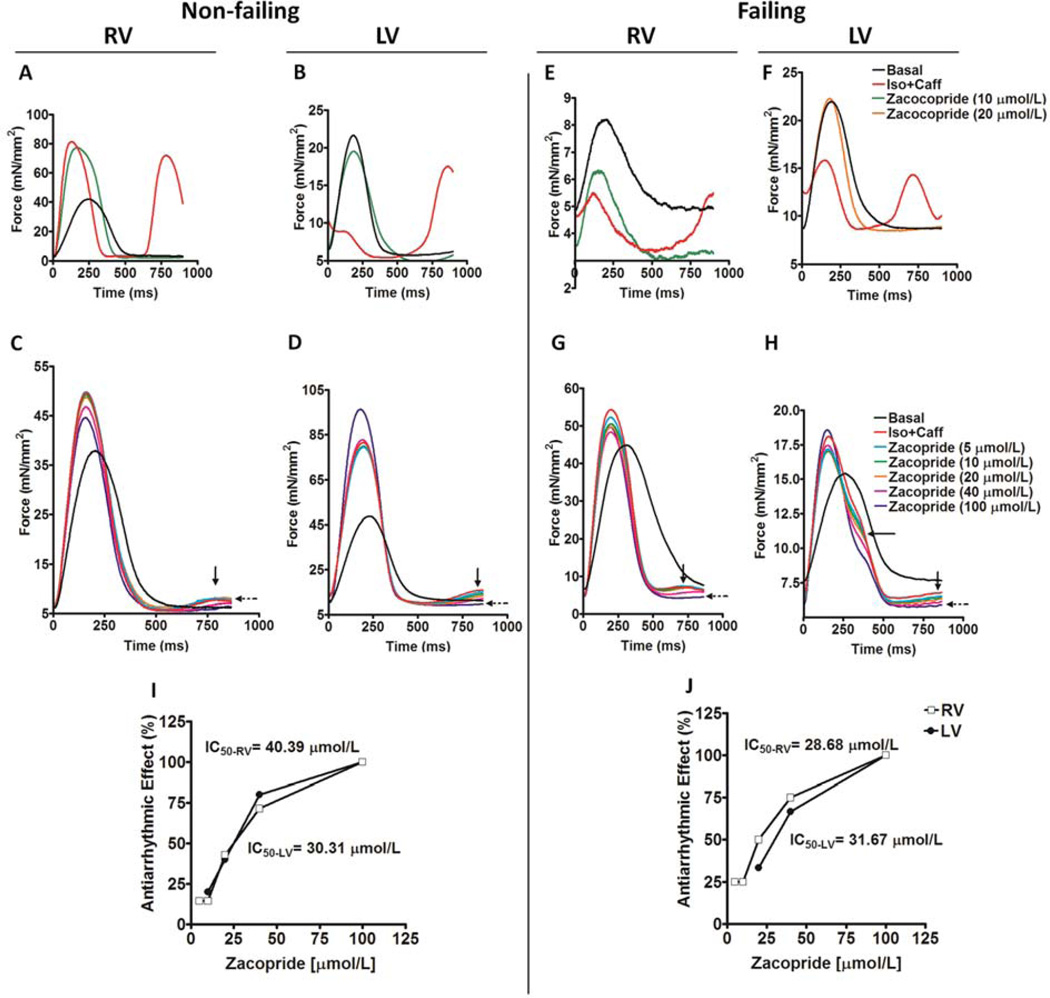
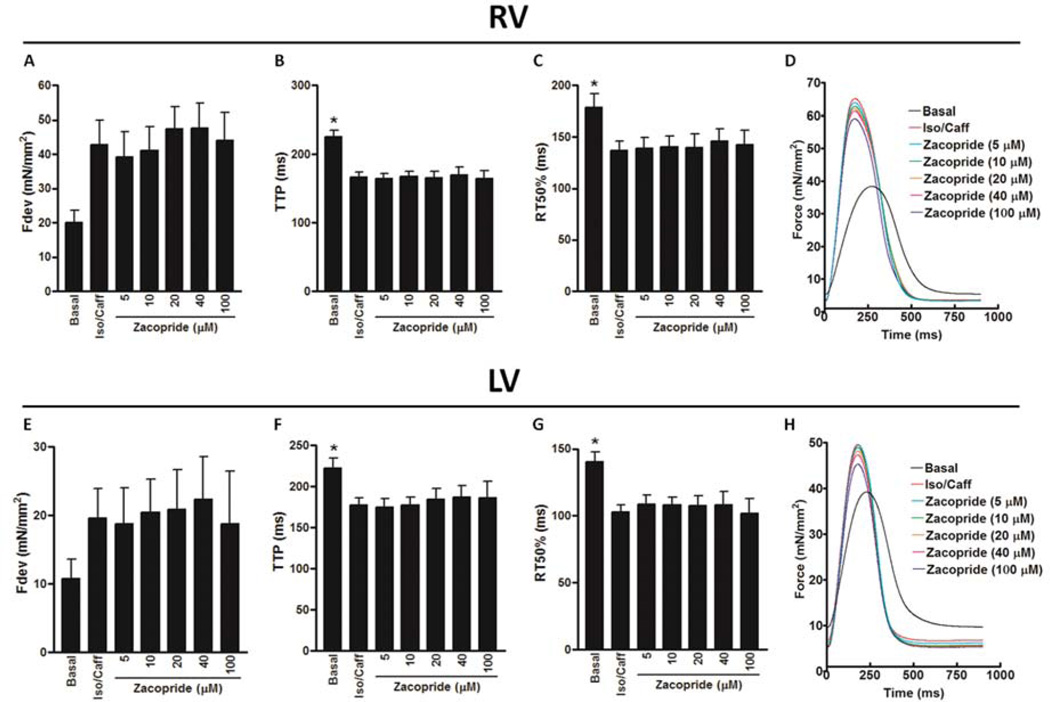
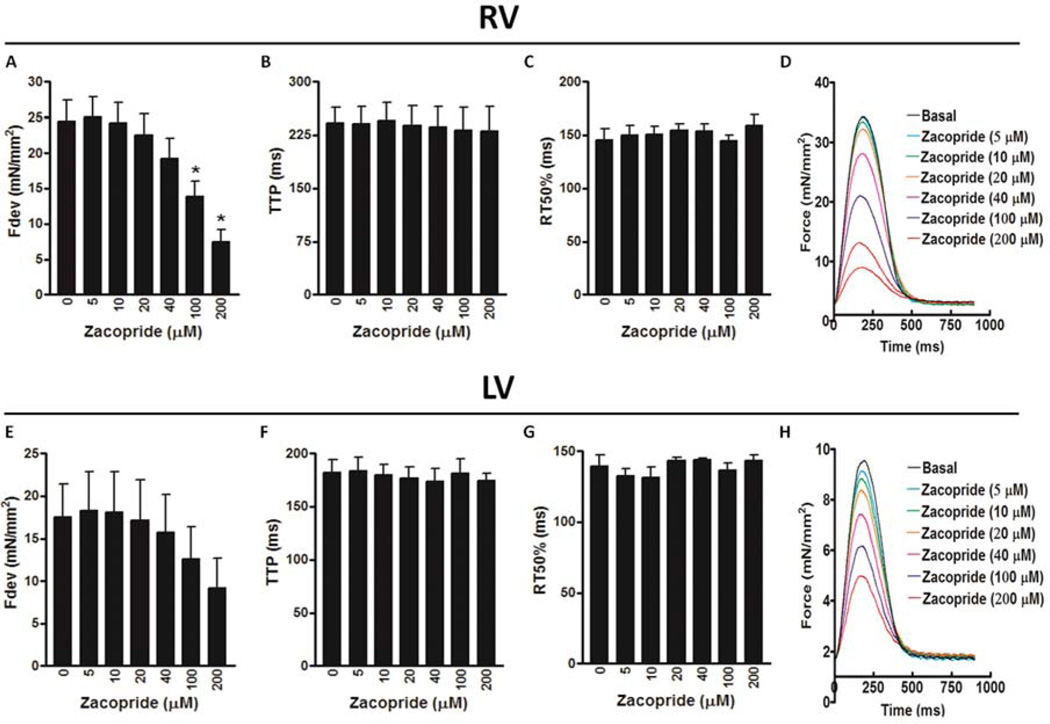
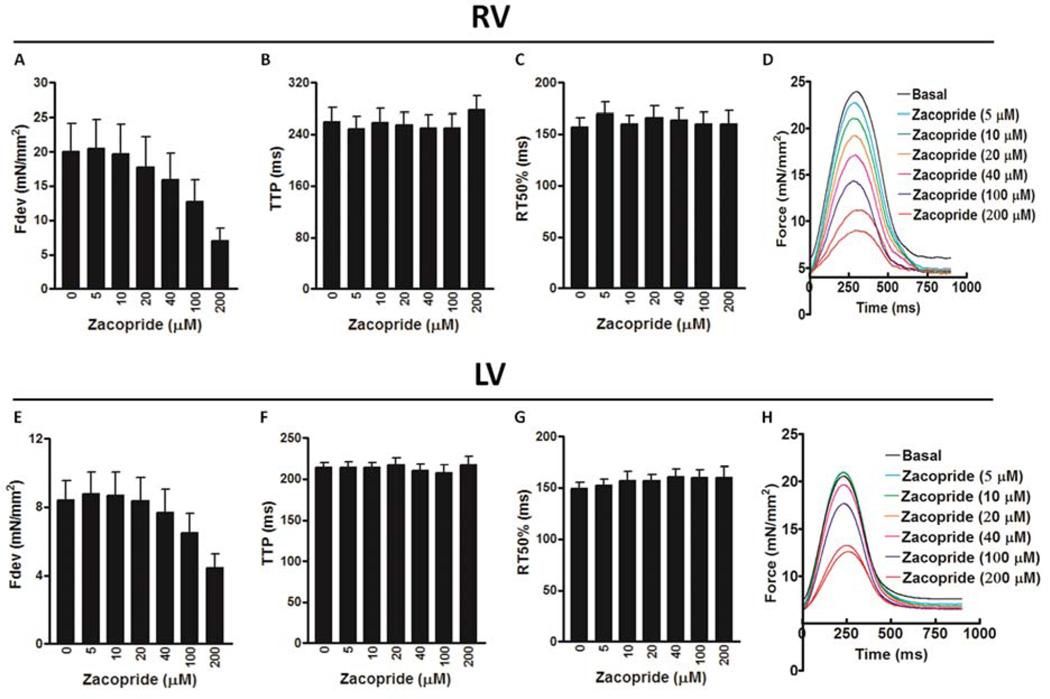
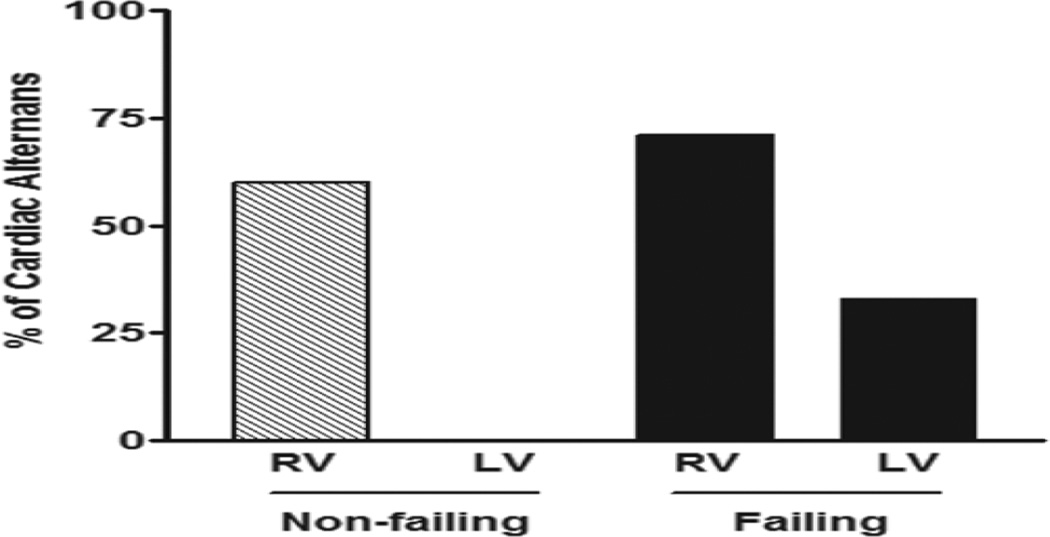
Ventricular tachycardia is the leading cause of sudden arrhythmic death in the U.S. Recently, the moderate IK1 channel activator, zacopride, was shown to suppress triggered ventricular tachycardia in rats. Nonetheless, concerns were raised about the possibility of pro-arrhythmic activity after IK1 channel stimulation based on the promising anti-arrhythmic strategy of IK1 blockade in other animal models. Therefore, the goal of the current study was to investigate the ex-vivo effects of zacopride on triggered arrhythmia and contractility in ventricular human myocardium in order to validate data that was solely obtained from animal models. Application of 100nmol/L isoproterenol and 0.5mmol/L caffeine led to triggered arrhythmia in isolated cardiac muscles from non-failing and end-stage failing hearts. However, the occurrence of arrhythmia in muscles of non-failing hearts was markedly higher than those of end-stage failing hearts. Interestingly, zacopride eliminated the ex-vivo triggered arrhythmia in these muscles of non-failing and failing hearts in a concentration-dependent manner, with an effective IC50 in the range of 28-40μmol/L. Conversely, in the absence of isoproterenol/caffeine, zacopride led to a negative inotropic effect in a concentration-dependent manner. Reduced cardiac contraction was clearly observed at high zacopride concentration of 200μmol/L, along with the occurrence of contractile alternans in muscles of non-failing and failing hearts. Zacopride shows promising antiarrhythmic effects against triggered arrhythmia in human ventricular myocardium. However, in the absence of Ca2+ overload/arrhythmia, zacopride, albeit at high concentrations, decreases the force of contraction and increases the likelihood of occurrence of contractile alternans, which may predispose the heart to contractile dysfunction and/or arrhythmia. Overall, our results represent a key step in translating this drug from the benchtop to the bedside in the research area.
Keywords: Contractility; Human heart; I(K1) channel; Triggered arrhythmia; Zacopride.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflicts-of-interest None.
Figures
Similar articles
-
Activation of IK1 channel by zacopride attenuates left ventricular remodeling in rats with myocardial infarction.J Cardiovasc Pharmacol. 2014 Oct;64(4):345-56. doi: 10.1097/FJC.0000000000000127. J Cardiovasc Pharmacol. 2014. Retraction in: J Cardiovasc Pharmacol. 2015 Mar;65(3):296. doi: 10.1097/01.fjc.0000462727.05737.2c. PMID: 25286360 Retracted.
-
The IK1/Kir2.1 channel agonist zacopride prevents and cures acute ischemic arrhythmias in the rat.PLoS One. 2017 May 18;12(5):e0177600. doi: 10.1371/journal.pone.0177600. eCollection 2017. PLoS One. 2017. PMID: 28542320 Free PMC article.
-
A novel discovery of IK1 channel agonist: zacopride selectively enhances IK1 current and suppresses triggered arrhythmias in the rat.J Cardiovasc Pharmacol. 2012 Jan;59(1):37-48. doi: 10.1097/FJC.0b013e3182350bcc. J Cardiovasc Pharmacol. 2012. PMID: 21921806
-
Tetramisole is a new IK1 channel agonist and exerts IK1 -dependent cardioprotective effects in rats.Pharmacol Res Perspect. 2022 Aug;10(4):e00992. doi: 10.1002/prp2.992. Pharmacol Res Perspect. 2022. PMID: 35880674 Free PMC article. Review.
-
Tedisamil: master switch of nature?Expert Opin Investig Drugs. 2001 Jan;10(1):129-38. doi: 10.1517/13543784.10.1.129. Expert Opin Investig Drugs. 2001. PMID: 11116286 Review.
Cited by
-
Human Myocardium Has a Robust α1A-Subtype Adrenergic Receptor Inotropic Response.J Cardiovasc Pharmacol. 2018 Sep;72(3):136-142. doi: 10.1097/FJC.0000000000000604. J Cardiovasc Pharmacol. 2018. PMID: 29923888 Free PMC article.
-
Force-frequency relationship and early relaxation kinetics are preserved upon sarcoplasmic blockade in human myocardium.Physiol Rep. 2018 Oct;6(20):e13898. doi: 10.14814/phy2.13898. Physiol Rep. 2018. PMID: 30350481 Free PMC article.
-
Etiology-dependent impairment of relaxation kinetics in right ventricular end-stage failing human myocardium.J Mol Cell Cardiol. 2018 Aug;121:81-93. doi: 10.1016/j.yjmcc.2018.07.005. Epub 2018 Jul 5. J Mol Cell Cardiol. 2018. PMID: 29981798 Free PMC article.
-
The network of cardiac KIR2.1: its function, cellular regulation, electrical signaling, diseases and new drug avenues.Naunyn Schmiedebergs Arch Pharmacol. 2024 Sep;397(9):6369-6389. doi: 10.1007/s00210-024-03116-5. Epub 2024 Apr 29. Naunyn Schmiedebergs Arch Pharmacol. 2024. PMID: 38683369 Free PMC article. Review.
-
Modeling heart failure in animal models for novel drug discovery and development.Expert Opin Drug Discov. 2019 Apr;14(4):355-363. doi: 10.1080/17460441.2019.1582636. Epub 2019 Mar 12. Expert Opin Drug Discov. 2019. PMID: 30861352 Free PMC article. Review.
References
-
- Bers DM. Excitation–Contraction Coupling and Cardiac Contractile Force. 2nd. Dordrecht: Springer; 2001.
-
- Pogwizd SM, McKenzie JP, Cain ME. Mechanisms underlying spontaneous and induced ventricular arrhythmias in patients with idiopathic dilated cardiomyopathy. Circulation. 1998;98:2404–2414. - PubMed
-
- Leenhardt A, Lucet V, Denjoy I, Grau F, Ngoc DD, Coumel P. Catecholaminergic polymorphic ventricular tachycardia in children. A 7-year follow-up of 21 patients. Circulation. 1995;91:1512–1519. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
