

Insights from Preclinical Choice Models on Treating Drug Addiction
- PMID: 27916279
- PMCID: PMC5258826
- DOI: 10.1016/j.tips.2016.11.002
Insights from Preclinical Choice Models on Treating Drug Addiction
Abstract
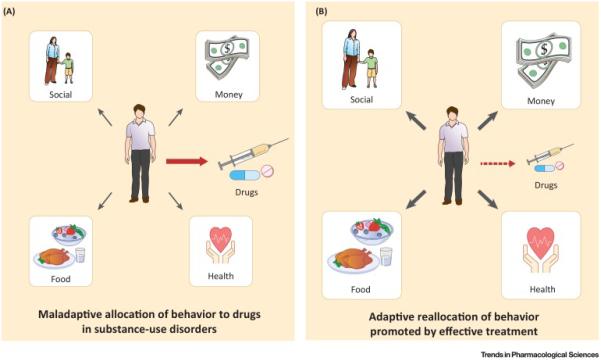
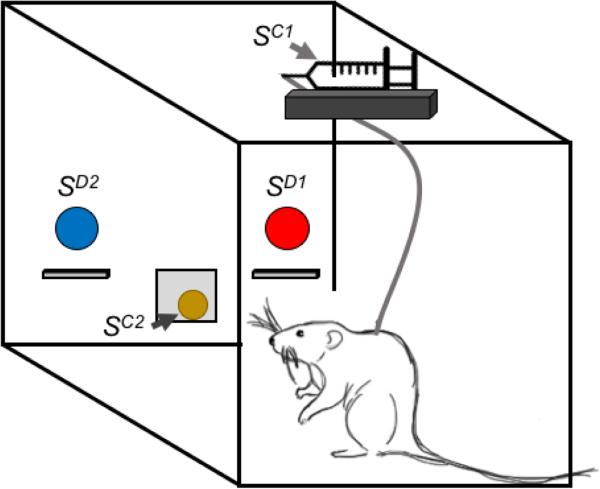
Substance-use disorders are a global public health problem that arises from behavioral misallocation between drug use and more adaptive behaviors maintained by nondrug alternatives (e.g., food or money). Preclinical drug self-administration procedures that incorporate a concurrently available nondrug reinforcer (e.g., food) provide translationally relevant and distinct dependent measures of behavioral allocation (i.e., to assess the relative reinforcing efficacy of the drug) and behavioral rate (i.e., to assess motor competence). In particular, preclinical drug versus food 'choice' procedures have produced increasingly concordant results with both human laboratory drug self-administration studies and double-blind placebo-controlled clinical trials. Accordingly, here we provide a heuristic framework of substance-use disorders based on a behavioral-centric perspective and recent insights from these preclinical choice procedures.
Keywords: addiction; choice; drug self-administration; preclinical model; substance-use disorder.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
References
-
- UNODC . World Drug Report 2015. United Nations Office on Drugs and Crime; 2015.
-
- Hall W, et al. Brain disease model of addiction: misplaced priorities? Lancet Psychiatry. 2015;2:867. - PubMed
-
- APA . Diagnositc and Statistical Manual Of Mental Disorders. 5th edn American Psychiatric Association; 2013.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
