

Novel non-invasive biological predictive index for liver fibrosis in hepatitis C virus genotype 4 patients
- PMID: 27917265
- PMCID: PMC5114475
- DOI: 10.4254/wjh.v8.i32.1392
Novel non-invasive biological predictive index for liver fibrosis in hepatitis C virus genotype 4 patients
Abstract
Aim: To investigate the diagnostic ability of a non-invasive biological marker to predict liver fibrosis in hepatitis C genotype 4 patients with high accuracy.
Methods: A cohort of 332 patients infected with hepatitis C genotype 4 was included in this cross-sectional study. Fasting plasma glucose, insulin, C-peptide, and angiotensin-converting enzyme serum levels were measured. Insulin resistance was mathematically calculated using the homeostasis model of insulin resistance (HOMA-IR).
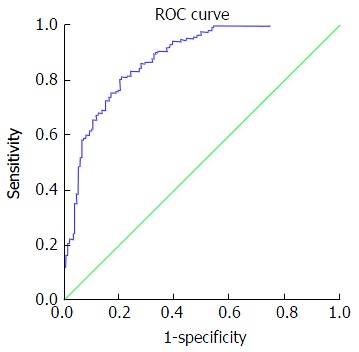
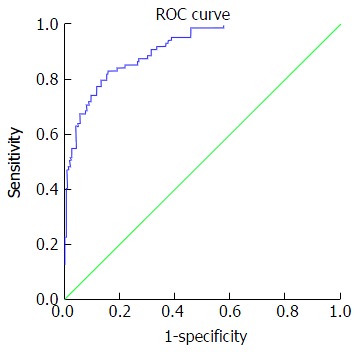
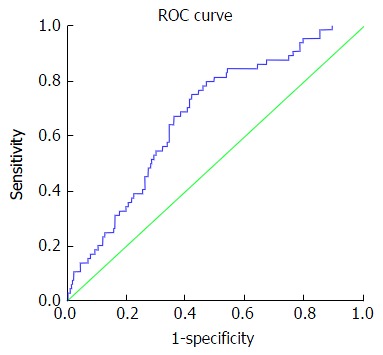
Results: Fibrosis stages were distributed based on Metavir score as follows: F0 = 43, F1 = 136, F2 = 64, F3 = 45 and F4 = 44. Statistical analysis relied upon reclassification of fibrosis stages into mild fibrosis (F0-F) = 179, moderate fibrosis (F2) = 64, and advanced fibrosis (F3-F4) = 89. Univariate analysis indicated that age, log aspartate amino transaminase, log HOMA-IR and log platelet count were independent predictors of liver fibrosis stage (P < 0.0001). A stepwise multivariate discriminant functional analysis was used to drive a discriminative model for liver fibrosis. Our index used cut-off values of ≥ 0.86 and ≤ -0.31 to diagnose advanced and mild fibrosis, respectively, with receiving operating characteristics of 0.91 and 0.88, respectively. The sensitivity, specificity, positive predictive value, negative predictive value and positive likelihood ratio were: 73%, 91%, 75%, 90% and 8.0 respectively for advanced fibrosis, and 67%, 88%, 84%, 70% and 4.9, respectively, for mild fibrosis.
Conclusion: Our predictive model is easily available and reproducible, and predicted liver fibrosis with acceptable accuracy.
Keywords: Age; Aspartate amino transaminase; Insulin resistance; Liver fibrosis; Platelets.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no competing interests.
Figures
Similar articles
-
Evaluation of diagnostic accuracy of APRI for prediction of fibrosis in hepatitis C patients.J Ayub Med Coll Abbottabad. 2008 Oct-Dec;20(4):122-6. J Ayub Med Coll Abbottabad. 2008. PMID: 19999223
-
Accuracy of simple biochemical tests in identifying liver fibrosis in patients co-infected with human immunodeficiency virus and hepatitis C virus.Clin Gastroenterol Hepatol. 2009 Mar;7(3):339-45. doi: 10.1016/j.cgh.2008.11.019. Epub 2008 Dec 3. Clin Gastroenterol Hepatol. 2009. PMID: 19171202
-
Predictors of liver fibrosis in HIV-infected patients with chronic hepatitis C virus (HCV) infection: assessment using transient elastometry and the role of HCV genotype 3.Clin Infect Dis. 2006 Apr 1;42(7):1032-9. doi: 10.1086/501021. Epub 2006 Feb 21. Clin Infect Dis. 2006. PMID: 16511772
-
[Comparative study of two models that use biochemical parameters for the non-invasive diagnosis of fibrosis in patients with hepatitis C].Med Clin (Barc). 2005 May 28;124(20):761-4. doi: 10.1157/13075845. Med Clin (Barc). 2005. PMID: 15927100 Spanish.
-
Limited reliability of five non-invasive biomarkers in predicting hepatic fibrosis in chronic HCV mono-infected patients opposed to METAVIR scoring.Pathol Res Pract. 2014 Dec;210(12):922-8. doi: 10.1016/j.prp.2014.07.005. Epub 2014 Jul 22. Pathol Res Pract. 2014. PMID: 25123964
References
-
- Lavanchy D. Evolving epidemiology of hepatitis C virus. Clin Microbiol Infect. 2011;17:107–115. - PubMed
-
- Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013;57:1333–1342. - PubMed
-
- Sievert W, Altraif I, Razavi HA, Abdo A, Ahmed EA, Alomair A, Amarapurkar D, Chen CH, Dou X, El Khayat H, et al. A systematic review of hepatitis C virus epidemiology in Asia, Australia and Egypt. Liver Int. 2011;31 Suppl 2:61–80. - PubMed
-
- Moreira RK. Hepatic stellate cells and liver fibrosis. Arch Pathol Lab Med. 2007;131:1728–1734. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
