

Phase I study of MRX34, a liposomal miR-34a mimic, administered twice weekly in patients with advanced solid tumors
- PMID: 27917453
- PMCID: PMC5893501
- DOI: 10.1007/s10637-016-0407-y
Phase I study of MRX34, a liposomal miR-34a mimic, administered twice weekly in patients with advanced solid tumors
Abstract
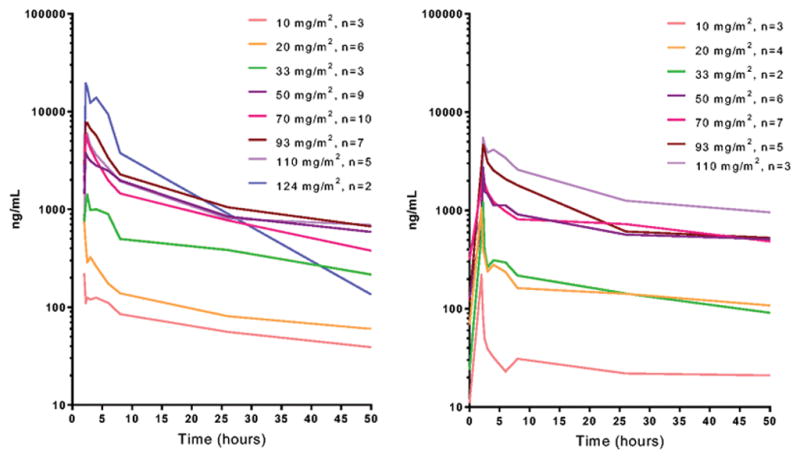
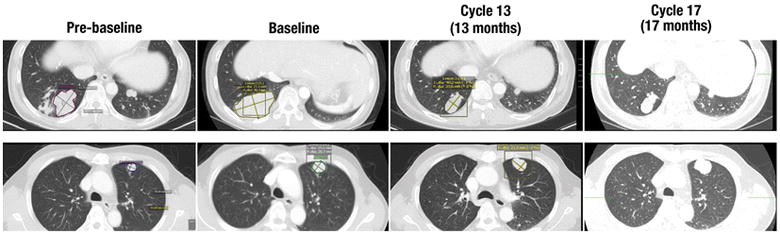
Purpose Naturally occurring tumor suppressor microRNA-34a (miR-34a) downregulates the expression of >30 oncogenes across multiple oncogenic pathways, as well as genes involved in tumor immune evasion, but is lost or under-expressed in many malignancies. This first-in-human, phase I study assessed the maximum tolerated dose (MTD), safety, pharmacokinetics, and clinical activity of MRX34, a liposomal miR-34a mimic, in patients with advanced solid tumors. Patients and Methods Adult patients with solid tumors refractory to standard treatment were enrolled in a standard 3 + 3 dose escalation trial. MRX34 was given intravenously twice weekly (BIW) for three weeks in 4-week cycles. Results Forty-seven patients with various solid tumors, including hepatocellular carcinoma (HCC; n = 14), were enrolled. Median age was 60 years, median prior therapies was 4 (range, 1-12), and most were Caucasian (68%) and male (57%). Most common adverse events (AEs) included fever (all grade %/G3%: 64/2), fatigue (57/13), back pain (57/11), nausea (49/2), diarrhea (40/11), anorexia (36/4), and vomiting (34/4). Laboratory abnormalities included lymphopenia (G3%/G4%: 23/9), neutropenia (13/11), thrombocytopenia (17/0), increased AST (19/4), hyperglycemia (13/2), and hyponatremia (19/2). Dexamethasone premedication was required to manage infusion-related AEs. The MTD for non-HCC patients was 110 mg/m2, with two patients experiencing dose-limiting toxicities of G3 hypoxia and enteritis at 124 mg/m2. The half-life was >24 h, and Cmax and AUC increased with increasing dose. One patient with HCC achieved a prolonged confirmed PR lasting 48 weeks, and four patients experienced SD lasting ≥4 cycles. Conclusion MRX34 treatment with dexamethasone premedication was associated with acceptable safety and showed evidence of antitumor activity in a subset of patients with refractory advanced solid tumors. The MTD for the BIW schedule was 110 mg/m2 for non-HCC and 93 mg/m2 for HCC patients. Additional dose schedules of MRX34 have been explored to improve tolerability.
Keywords: Advanced solid tumors; Experimental therapeutics; Phase I trial; miR-34a; microRNA.
Figures
References
-
- Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell. 2004;116:281–97. - PubMed
-
- Calin GA, Croce CM. MicroRNA signatures in human cancers. Nat Rev Cancer. 2006;6:857–66. - PubMed
-
- Esquela-Kerscher A, Slack FJ. Oncomirs - microRNAs with a role in cancer. Nat Rev Cancer. 2006;6:259–69. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
