

What Is the Best Treatment of Locally Advanced Nasopharyngeal Carcinoma? An Individual Patient Data Network Meta-Analysis
- PMID: 27918720
- PMCID: PMC5791836
- DOI: 10.1200/JCO.2016.67.4119
What Is the Best Treatment of Locally Advanced Nasopharyngeal Carcinoma? An Individual Patient Data Network Meta-Analysis
Abstract
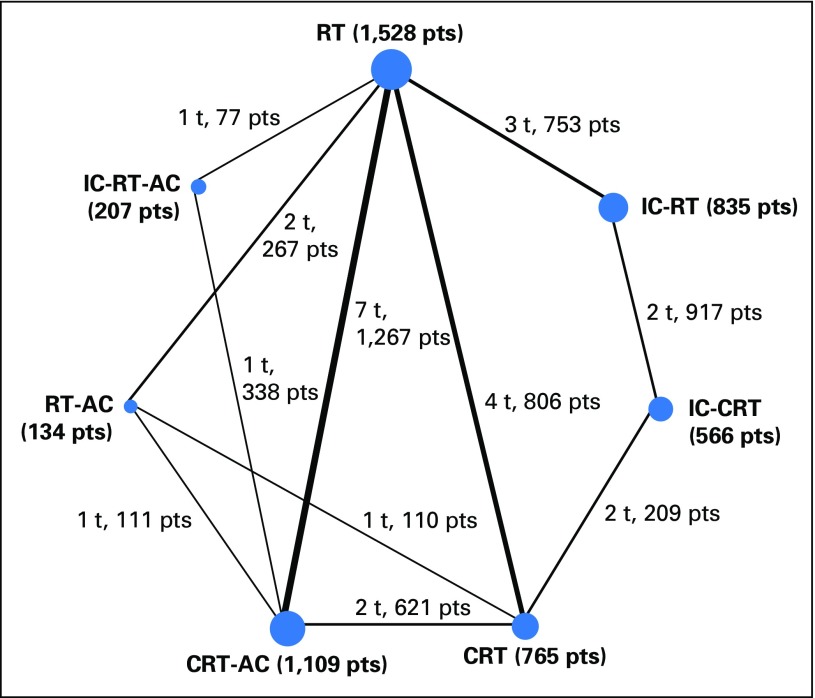
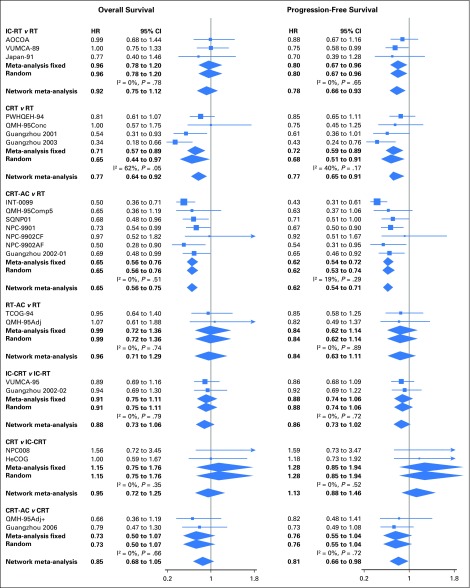
Purpose The role of adjuvant chemotherapy (AC) or induction chemotherapy (IC) in the treatment of locally advanced nasopharyngeal carcinoma is controversial. The individual patient data from the Meta-Analysis of Chemotherapy in Nasopharynx Carcinoma database were used to compare all available treatments. Methods All randomized trials of radiotherapy (RT) with or without chemotherapy in nonmetastatic nasopharyngeal carcinoma were considered. Overall, 20 trials and 5,144 patients were included. Treatments were grouped into seven categories: RT alone (RT), IC followed by RT (IC-RT), RT followed by AC (RT-AC), IC followed by RT followed by AC (IC-RT-AC), concomitant chemoradiotherapy (CRT), IC followed by CRT (IC-CRT), and CRT followed by AC (CRT-AC). P-score was used to rank the treatments. Fixed- and random-effects frequentist network meta-analysis models were applied. Results The three treatments with the highest probability of benefit on overall survival (OS) were CRT-AC, followed by CRT and IC-CRT, with respective hazard ratios (HRs [95% CIs]) compared with RT alone of 0.65 (0.56 to 0.75), 0.77 (0.64 to 0.92), and 0.81 (0.63 to 1.04). HRs (95% CIs) of CRT-AC compared with CRT for OS, progression-free survival (PFS), locoregional control, and distant control (DC) were, respectively, 0.85 (0.68 to 1.05), 0.81 (0.66 to 0.98), 0.70 (0.48 to 1.02), and 0.87 (0.61 to 1.25). IC-CRT ranked second for PFS and the best for DC. CRT never ranked first. HRs of CRT compared with IC-CRT for OS, PFS, locoregional control, and DC were, respectively, 0.95 (0.72 to 1.25), 1.13 (0.88 to 1.46), 1.05 (0.70 to 1.59), and 1.55 (0.94 to 2.56). Regimens with more chemotherapy were associated with increased risk of acute toxicity. Conclusion The addition of AC to CRT achieved the highest survival benefit and consistent improvement for all end points. The addition of IC to CRT achieved the highest effect on DC.
Figures
Comment in
-
Multiple-Treatments Meta-Analysis: Are the Conclusions Supported by the Data?J Clin Oncol. 2017 Feb 10;35(5):565-566. doi: 10.1200/JCO.2016.70.4775. Epub 2016 Dec 5. J Clin Oncol. 2017. PMID: 27918722 No abstract available.
-
[The best multimodal treatment for locally advanced nasopharyngeal carcinoma : An update of the MAC-NPC data].Strahlenther Onkol. 2017 Oct;193(10):856-858. doi: 10.1007/s00066-017-1189-7. Strahlenther Onkol. 2017. PMID: 28812097 German. No abstract available.
References
-
- Blanchard P, Lee A, Marguet S, et al. Chemotherapy and radiotherapy in nasopharyngeal carcinoma: An update of the MAC-NPC meta-analysis. Lancet Oncol. 2015;16:645–655. - PubMed
-
- Chan ATC, Grégoire V, Lefebvre J-L, et al. Nasopharyngeal cancer: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012;23:vii83–vii85. (suppl 7) - PubMed
-
- National Comprehensive Cancer Network: NCCN Guidelines - Head and Neck Cancers (version 2.2016). Fort Washington, PA, National Comprehensive Cancer Network. - PubMed
-
- Lee AWM, Ng WT, Chan LLK, et al. Evolution of treatment for nasopharyngeal cancer--success and setback in the intensity-modulated radiotherapy era. Radiother Oncol. 2014;110:377–384. - PubMed
-
- Blanchard P, Hill C, Guihenneuc-Jouyaux C, et al. Mixed treatment comparison meta-analysis of altered fractionated radiotherapy and chemotherapy in head and neck cancer. J Clin Epidemiol. 2011;64:985–992. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
