

Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study
- PMID: 27918777
- PMCID: PMC6103527
- DOI: 10.1001/jamaoncol.2016.5688
Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study
Erratum in
-
Additional Study Contributors Reported After Publication.JAMA Oncol. 2017 Mar 1;3(3):418. doi: 10.1001/jamaoncol.2017.0098. JAMA Oncol. 2017. PMID: 28278330 No abstract available.
Abstract
Importance: Cancer is the second leading cause of death worldwide. Current estimates on the burden of cancer are needed for cancer control planning.
Objective: To estimate mortality, incidence, years lived with disability (YLDs), years of life lost (YLLs), and disability-adjusted life-years (DALYs) for 32 cancers in 195 countries and territories from 1990 to 2015.
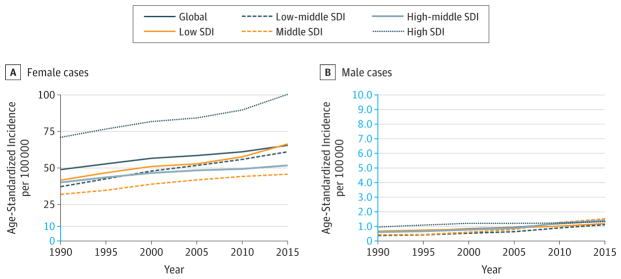
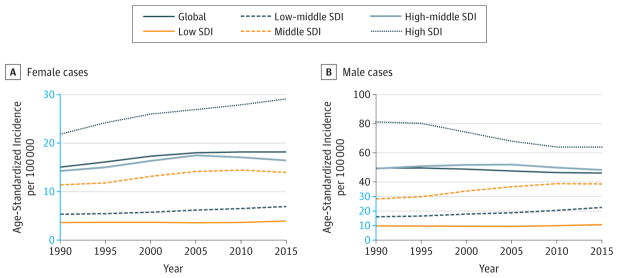
Evidence review: Cancer mortality was estimated using vital registration system data, cancer registry incidence data (transformed to mortality estimates using separately estimated mortality to incidence [MI] ratios), and verbal autopsy data. Cancer incidence was calculated by dividing mortality estimates through the modeled MI ratios. To calculate cancer prevalence, MI ratios were used to model survival. To calculate YLDs, prevalence estimates were multiplied by disability weights. The YLLs were estimated by multiplying age-specific cancer deaths by the reference life expectancy. DALYs were estimated as the sum of YLDs and YLLs. A sociodemographic index (SDI) was created for each location based on income per capita, educational attainment, and fertility. Countries were categorized by SDI quintiles to summarize results.
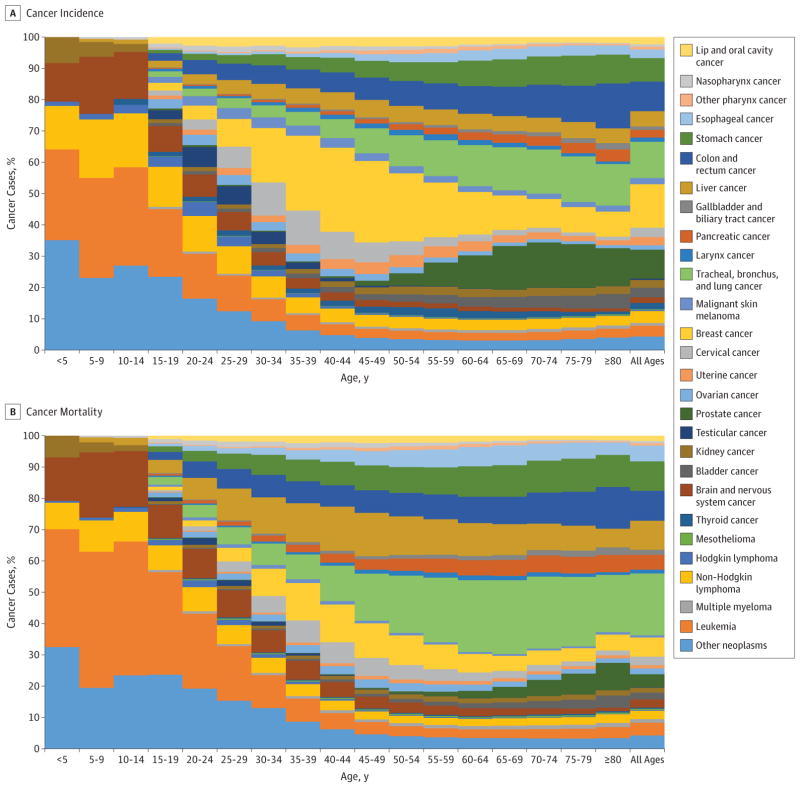
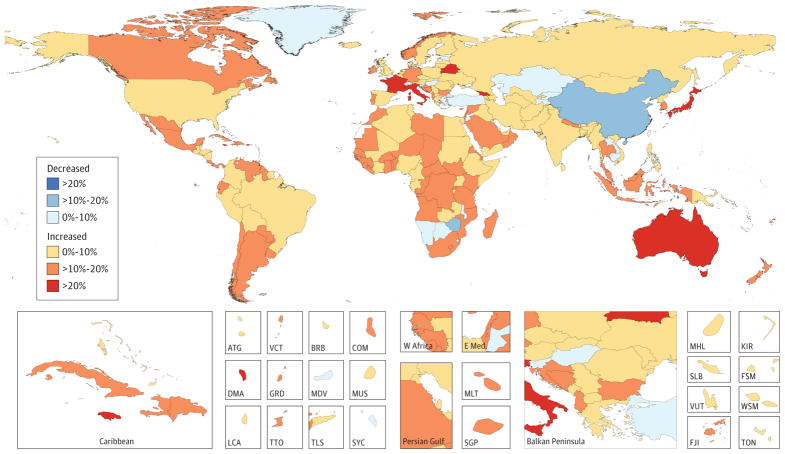
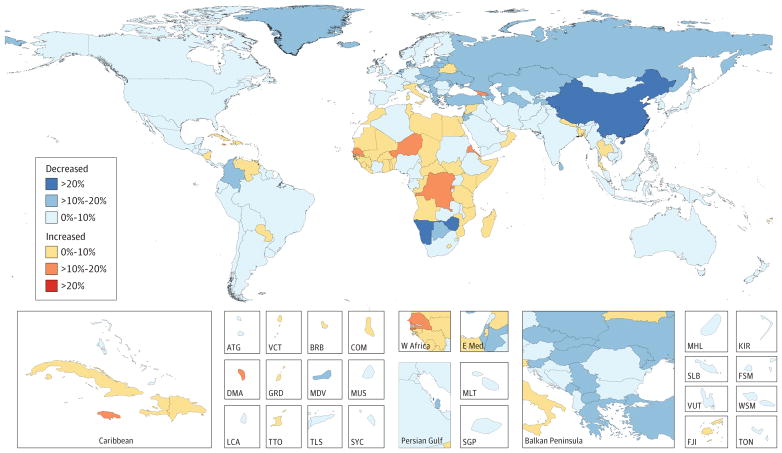
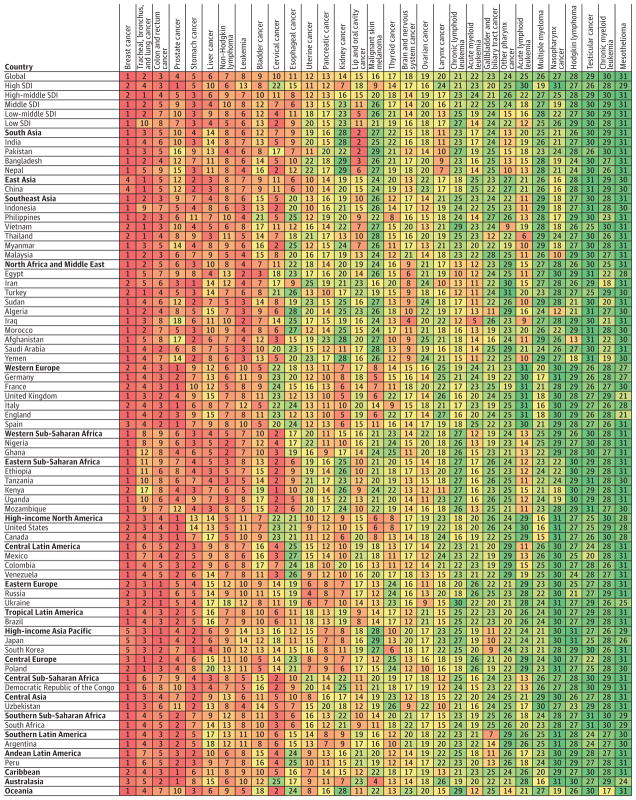
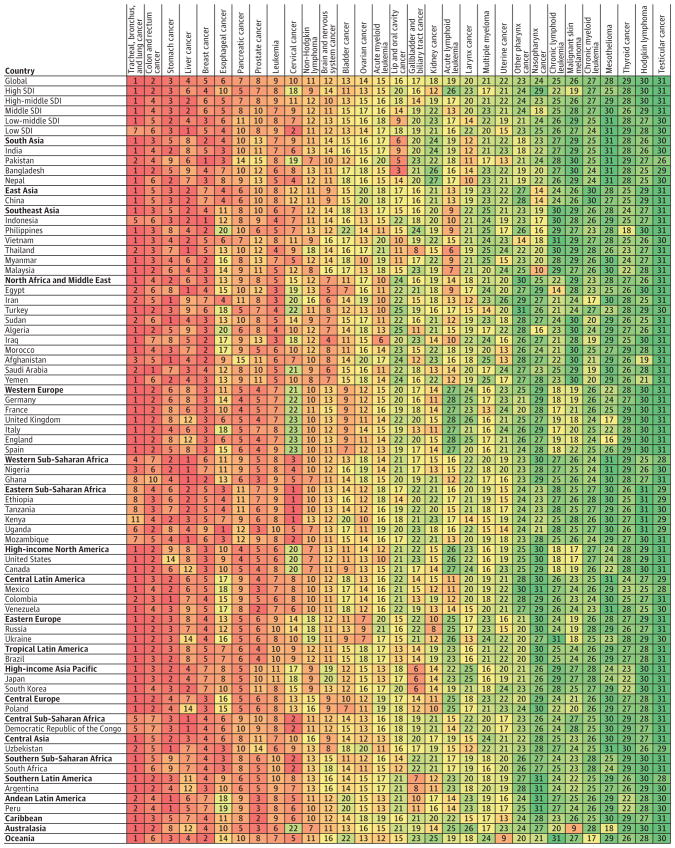
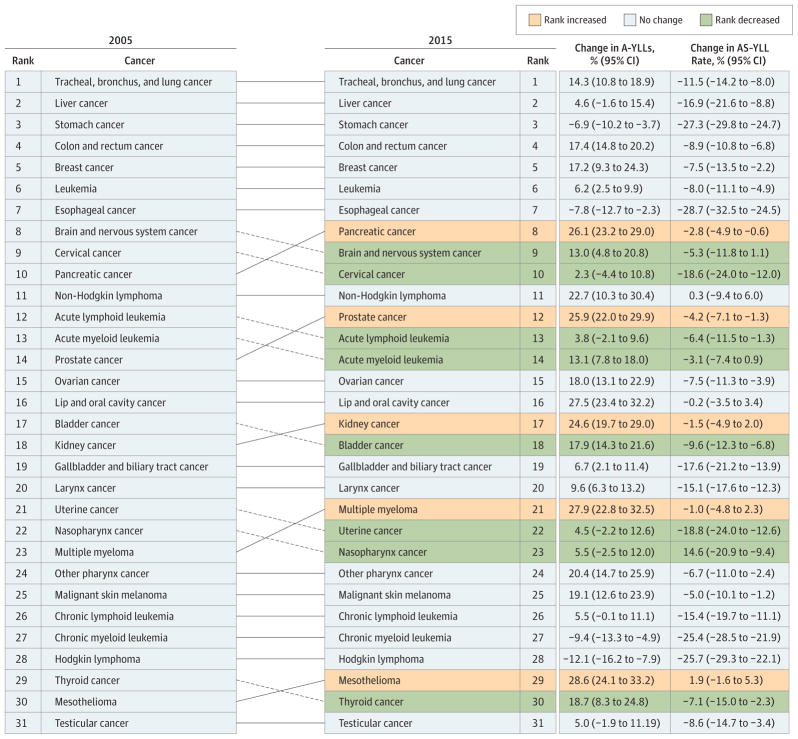
Findings: In 2015, there were 17.5 million cancer cases worldwide and 8.7 million deaths. Between 2005 and 2015, cancer cases increased by 33%, with population aging contributing 16%, population growth 13%, and changes in age-specific rates contributing 4%. For men, the most common cancer globally was prostate cancer (1.6 million cases). Tracheal, bronchus, and lung cancer was the leading cause of cancer deaths and DALYs in men (1.2 million deaths and 25.9 million DALYs). For women, the most common cancer was breast cancer (2.4 million cases). Breast cancer was also the leading cause of cancer deaths and DALYs for women (523 000 deaths and 15.1 million DALYs). Overall, cancer caused 208.3 million DALYs worldwide in 2015 for both sexes combined. Between 2005 and 2015, age-standardized incidence rates for all cancers combined increased in 174 of 195 countries or territories. Age-standardized death rates (ASDRs) for all cancers combined decreased within that timeframe in 140 of 195 countries or territories. Countries with an increase in the ASDR due to all cancers were largely located on the African continent. Of all cancers, deaths between 2005 and 2015 decreased significantly for Hodgkin lymphoma (-6.1% [95% uncertainty interval (UI), -10.6% to -1.3%]). The number of deaths also decreased for esophageal cancer, stomach cancer, and chronic myeloid leukemia, although these results were not statistically significant.
Conclusion and relevance: As part of the epidemiological transition, cancer incidence is expected to increase in the future, further straining limited health care resources. Appropriate allocation of resources for cancer prevention, early diagnosis, and curative and palliative care requires detailed knowledge of the local burden of cancer. The GBD 2015 study results demonstrate that progress is possible in the war against cancer. However, the major findings also highlight an unmet need for cancer prevention efforts, including tobacco control, vaccination, and the promotion of physical activity and a healthy diet.
Conflict of interest statement
Figures
Comment in
-
Cancer prevention from the perspective of global cancer burden patterns.J Thorac Dis. 2017 Mar;9(3):448-451. doi: 10.21037/jtd.2017.02.75. J Thorac Dis. 2017. PMID: 28449441 Free PMC article. No abstract available.
-
Exclusion of Kaposi Sarcoma From Analysis of Cancer Burden.JAMA Oncol. 2017 Oct 1;3(10):1429. doi: 10.1001/jamaoncol.2016.7092. JAMA Oncol. 2017. PMID: 28662221 Free PMC article. No abstract available.
-
Exclusion of Kaposi Sarcoma From Analysis of Cancer Burden-Reply.JAMA Oncol. 2017 Oct 1;3(10):1429-1430. doi: 10.1001/jamaoncol.2017.1747. JAMA Oncol. 2017. PMID: 28662223 No abstract available.
References
-
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1459–1544. - PMC - PubMed
-
- Grady D. A sickened body as cancer weapon. The New York Times. 2016 Jul 30;
-
- Horton S, Gauvreau CL. Cancer in Low- and Middle-Income Countries: An Economic Overview. In: Gelband H, Jha P, Sankaranarayanan R, Horton S, editors. Cancer: Disease Control Priorities. 3. Vol. 3. Washington, DC: The International Bank for Reconstruction and Development/The World Bank; 2015. [Accessed July 31, 2016]. http://www.ncbi.nlm.nih.gov/books/NBK343620/ - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
