

Dual Health Care System Use and High-Risk Prescribing in Patients With Dementia: A National Cohort Study
- PMID: 27919104
- PMCID: PMC8048048
- DOI: 10.7326/M16-0551
Dual Health Care System Use and High-Risk Prescribing in Patients With Dementia: A National Cohort Study
Abstract
Background: Recent federal policy changes attempt to expand veterans' access to providers outside the Department of Veterans Affairs (VA). Receipt of prescription medications across unconnected systems of care may increase the risk for unsafe prescribing, particularly in persons with dementia.
Objective: To investigate the association between dual health care system use and potentially unsafe medication (PUM) prescribing.
Design: Retrospective cohort study.
Setting: National VA outpatient care facilities in 2010.
Participants: 75 829 veterans with dementia who were continuously enrolled in Medicare from 2007 to 2010; 80% were VA-only users, and 20% were VA-Medicare Part D (dual) users.
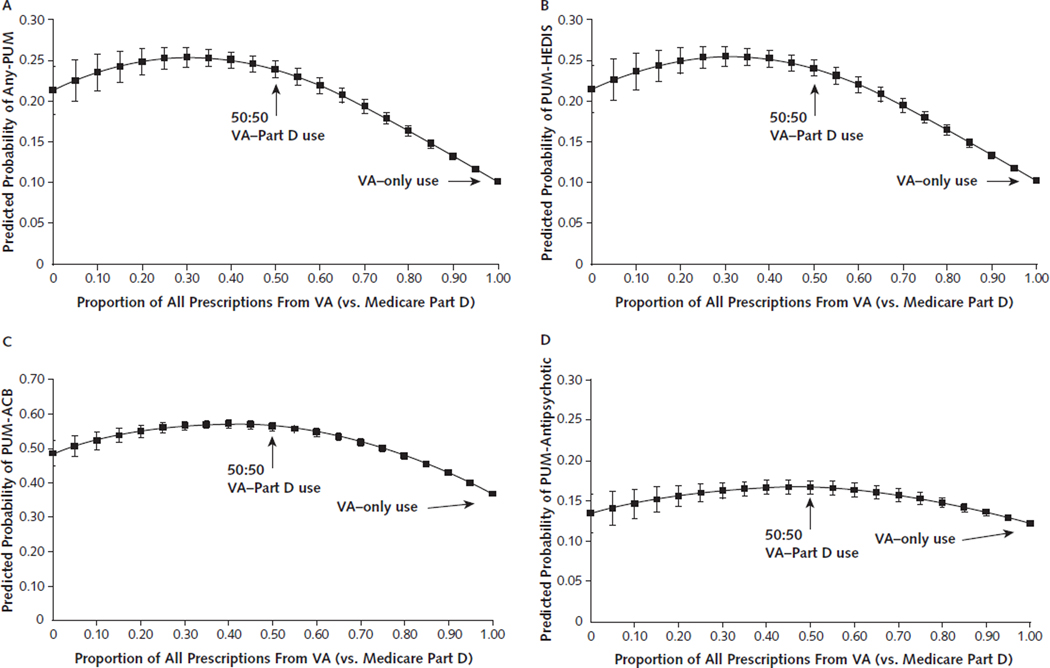
Measurements: Augmented inverse propensity weighting was used to estimate the effect of dual-system versus VA-only prescribing on 4 indicators of PUM prescribing in 2010: any exposure to Healthcare Effectiveness Data and Information Set (HEDIS) high-risk medication in older adults (PUM-HEDIS), any daily exposure to prescriptions with a cumulative Anticholinergic Cognitive Burden (ACB) score of 3 or higher (PUM-ACB), any antipsychotic prescription (PUM-antipsychotic), and any PUM exposure (any-PUM). The annual number of days of each PUM exposure was also examined.
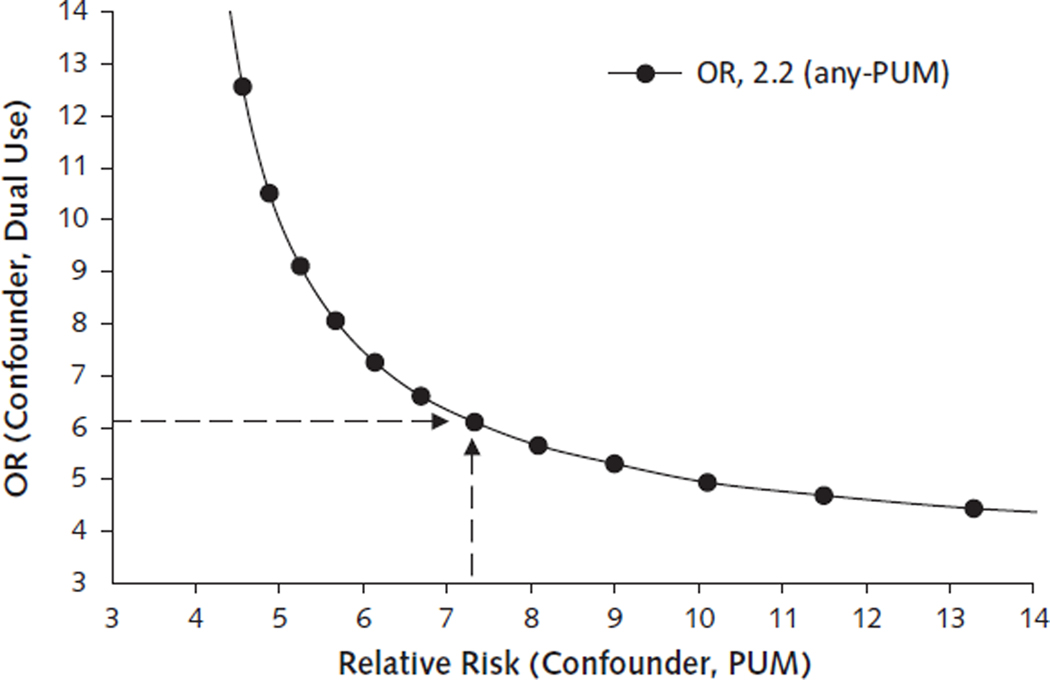
Results: Compared with VA-only users, dual users had more than double the odds of exposure to any-PUM (odds ratio [OR], 2.2 [95% CI, 2.2 to 2.3]), PUM-HEDIS (OR, 2.4 [CI, 2.2 to 2.8]), and PUM-ACB (OR, 2.1 [CI, 2.0 to 2.2]). The odds of PUM-antipsychotic exposure were also greater in dual users (OR, 1.5 [CI, 1.4 to 1.6]). Dual users had an adjusted average of 44.1 additional days of any-PUM exposure (CI, 37.2 to 45.0 days).
Limitation: Observational study design of veteran outpatients only.
Conclusion: Among veterans with dementia, rates of PUM prescribing are significantly higher among dual-system users than with VA-only users.
Primary funding source: U.S. Department of Veterans Affairs.
Figures
Comment in
-
The Veterans Affairs Pharmacy System: Perfectly Designed to Achieve the Outcomes It Gets.Ann Intern Med. 2017 Feb 7;166(3):221-222. doi: 10.7326/M16-2590. Epub 2016 Dec 6. Ann Intern Med. 2017. PMID: 27919102 No abstract available.
Summary for patients in
-
Dual Health Care System Use and Unsafe Medication Prescribing in Veterans With Dementia.Ann Intern Med. 2017 Feb 7;166(3). doi: 10.7326/P16-9026. Epub 2016 Dec 6. Ann Intern Med. 2017. PMID: 27919105 No abstract available.
References
-
- World Health Organization. Dementia: A Public Health Priority. Geneva, Switzerland.
-
- Cooley SG, Asthana S. Dementia care for veterans: Enhancing comprehensive, coordinated services. Generations. 2011;34(42):57–63.
-
- U.S. Department of Health and Human Services. Healthy People 2020. Washington, DC: Office of Disease Prevention and Health Promotion; 2012.
-
- Callahan CM, Boustani MA, Unverzagt FW, Austrom MG, Damush TM, Perkins AJ, et al. Effectiveness of collaborative care for older adults with Alzheimer disease in primary care: a randomized controlled trial. JAMA. 2006;295(18):2148–57. - PubMed
-
- Bynum JP, Rabins PV, Weller W, Niefeld M, Anderson GF, Wu AW. The relationship between a dementia diagnosis, chronic illness, medicare expenditures, and hospital use. J Am Geriatr Soc. 2004;52(2):187–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous