

Proton therapy - Present and future
- PMID: 27919760
- PMCID: PMC5303653
- DOI: 10.1016/j.addr.2016.11.006
Proton therapy - Present and future
Abstract
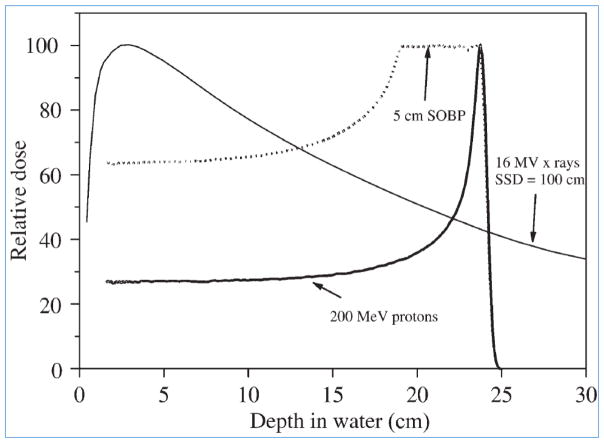
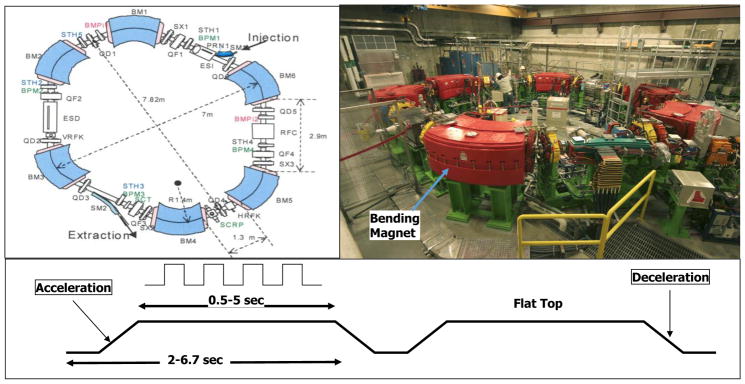
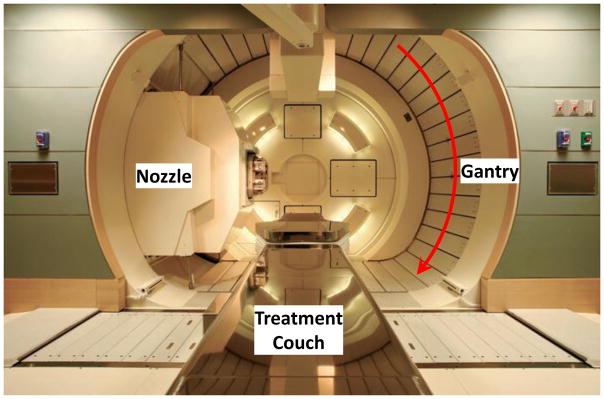
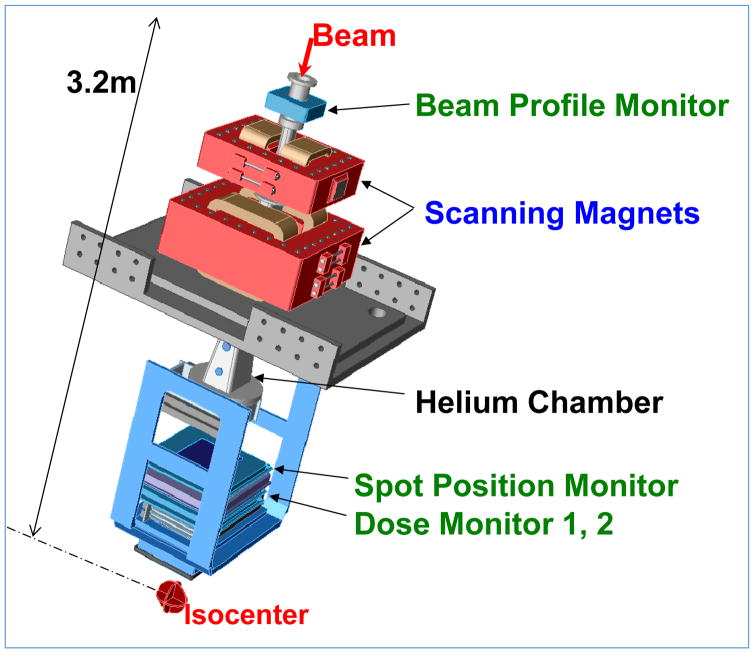
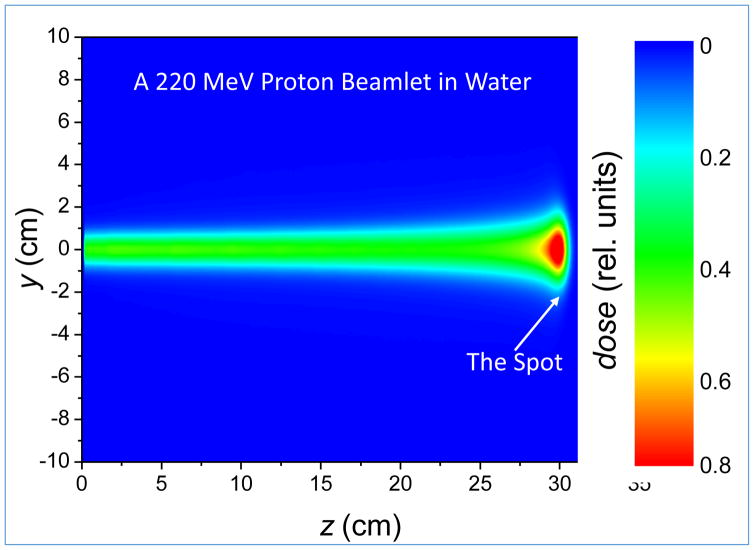
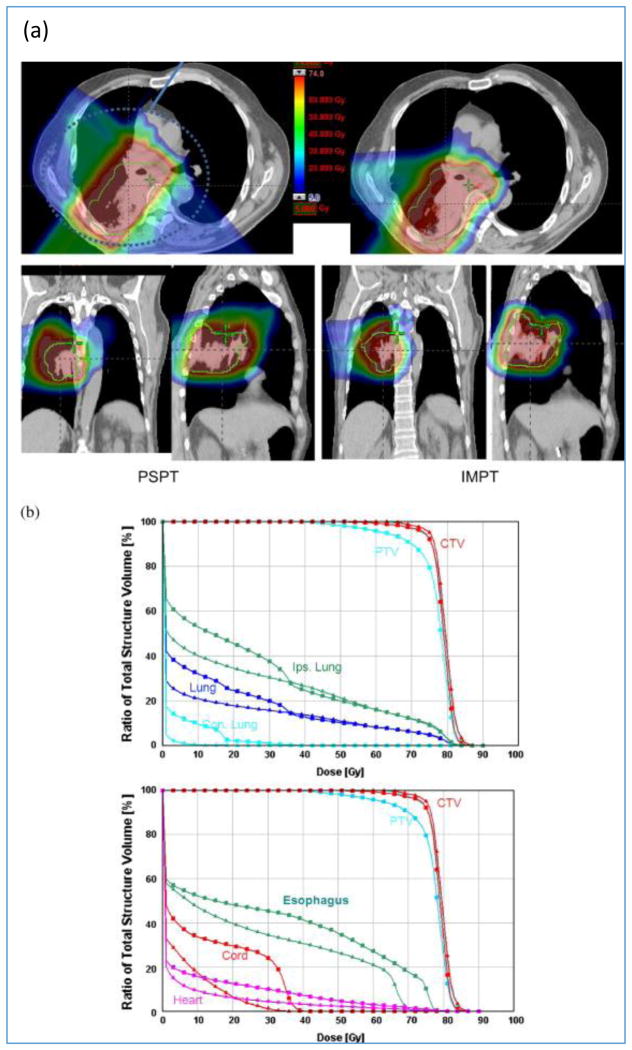
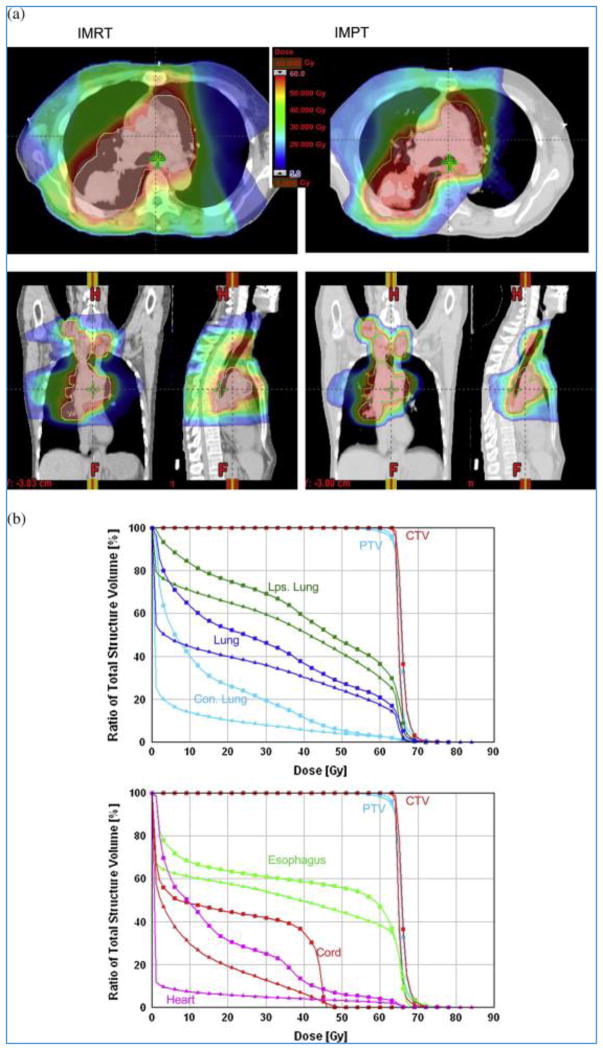
In principle, proton therapy offers a substantial clinical advantage over conventional photon therapy. This is because of the unique depth-dose characteristics of protons, which can be exploited to achieve significant reductions in normal tissue doses proximal and distal to the target volume. These may, in turn, allow escalation of tumor doses and greater sparing of normal tissues, thus potentially improving local control and survival while at the same time reducing toxicity and improving quality of life. Protons, accelerated to therapeutic energies ranging from 70 to 250MeV, typically with a cyclotron or a synchrotron, are transported to the treatment room where they enter the treatment head mounted on a rotating gantry. The initial thin beams of protons are spread laterally and longitudinally and shaped appropriately to deliver treatments. Spreading and shaping can be achieved by electro-mechanical means to treat the patients with "passively-scattered proton therapy" (PSPT) or using magnetic scanning of thin "beamlets" of protons of a sequence of initial energies. The latter technique can be used to treat patients with optimized intensity modulated proton therapy (IMPT), the most powerful proton modality. Despite the high potential of proton therapy, the clinical evidence supporting the broad use of protons is mixed. It is generally acknowledged that proton therapy is safe, effective and recommended for many types of pediatric cancers, ocular melanomas, chordomas and chondrosarcomas. Although promising results have been and continue to be reported for many other types of cancers, they are based on small studies. Considering the high cost of establishing and operating proton therapy centers, questions have been raised about their cost effectiveness. General consensus is that there is a need to conduct randomized trials and/or collect outcomes data in multi-institutional registries to unequivocally demonstrate the advantage of protons. Treatment planning and plan evaluation of PSPT and IMPT require special considerations compared to the processes used for photon treatment planning. The differences in techniques arise from the unique physical properties of protons but are also necessary because of the greater vulnerability of protons to uncertainties, especially from inter- and intra-fractional variations in anatomy. These factors must be considered in designing as well as evaluating treatment plans. In addition to anatomy variations, other sources of uncertainty in dose delivered to the patient include the approximations and assumptions of models used for computing dose distributions for planning of treatments. Furthermore, the relative biological effectiveness (RBE) of protons is simplistically assumed to have a constant value of 1.1. In reality, the RBE is variable and a complex function of the energy of protons, dose per fraction, tissue and cell type, end point, etc. These uncertainties, approximations and current technological limitations of proton therapy may limit the achievement of its true potential. Ongoing research is aimed at better understanding the consequences of the various uncertainties on proton therapy and reducing the uncertainties through image-guidance, adaptive radiotherapy, further study of biological properties of protons and the development of novel dose computation and optimization methods. However, residual uncertainties will remain in spite of the best efforts. To increase the resilience of dose distributions in the face of uncertainties and improve our confidence in dose distributions seen on treatment plans, robust optimization techniques are being developed and implemented. We assert that, with such research, proton therapy will be a commonly applied radiotherapy modality for most types of solid cancers in the near future.
Keywords: Intensity-modulated proton therapy; Particle therapy; Proton therapy; Radiation therapy.
Copyright © 2016 Elsevier B.V. All rights reserved.
Figures




References
-
- Jones DTL. Present status and future trends of heavy particle radiotherapy. In: Baron E, Lieuvin M, editors. Cyclotrons and Their Applications 1998. Institute of Physics Publishing; Bristol, UK: 1999. pp. 13–20.
-
- Wilson RR. Radiological use of fast protons. Radiology. 1946;47:487–491. - PubMed
-
- Lawrence JH, Tobias CA, Born JL, Mc CR, Roberts JE, Anger HO, Low-Beer BV, Huggins CB. Pituitary irradiation with high-energy proton beams: a preliminary report. Cancer research. 1958;18:121–134. - PubMed
-
- Suit HD, Goitein M, Tepper J, Koehler AM, Schmidt RA, Schneider R. Explorotory study of proton radiation therapy using large field techniques and fractionated dose schedules. Cancer. 1975;35:1646–1657. - PubMed
-
- Coutrakon G, Hubbard J, Johanning J, Maudsley G, Slaton T, Morton P. A performance study of the Loma Linda proton medical accelerator. Med Phys. 1994;21:1691–1701. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
