

Clinic Blood Pressure Underestimates Ambulatory Blood Pressure in an Untreated Employer-Based US Population: Results From the Masked Hypertension Study
- PMID: 27920072
- PMCID: PMC5151173
- DOI: 10.1161/CIRCULATIONAHA.116.023404
Clinic Blood Pressure Underestimates Ambulatory Blood Pressure in an Untreated Employer-Based US Population: Results From the Masked Hypertension Study
Abstract
Background: Ambulatory blood pressure (ABP) is consistently superior to clinic blood pressure (CBP) as a predictor of cardiovascular morbidity and mortality risk. A common perception is that ABP is usually lower than CBP. The relationship of the CBP minus ABP difference to age has not been examined in the United States.
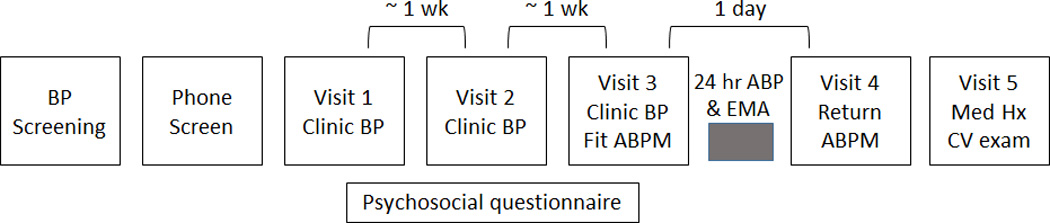
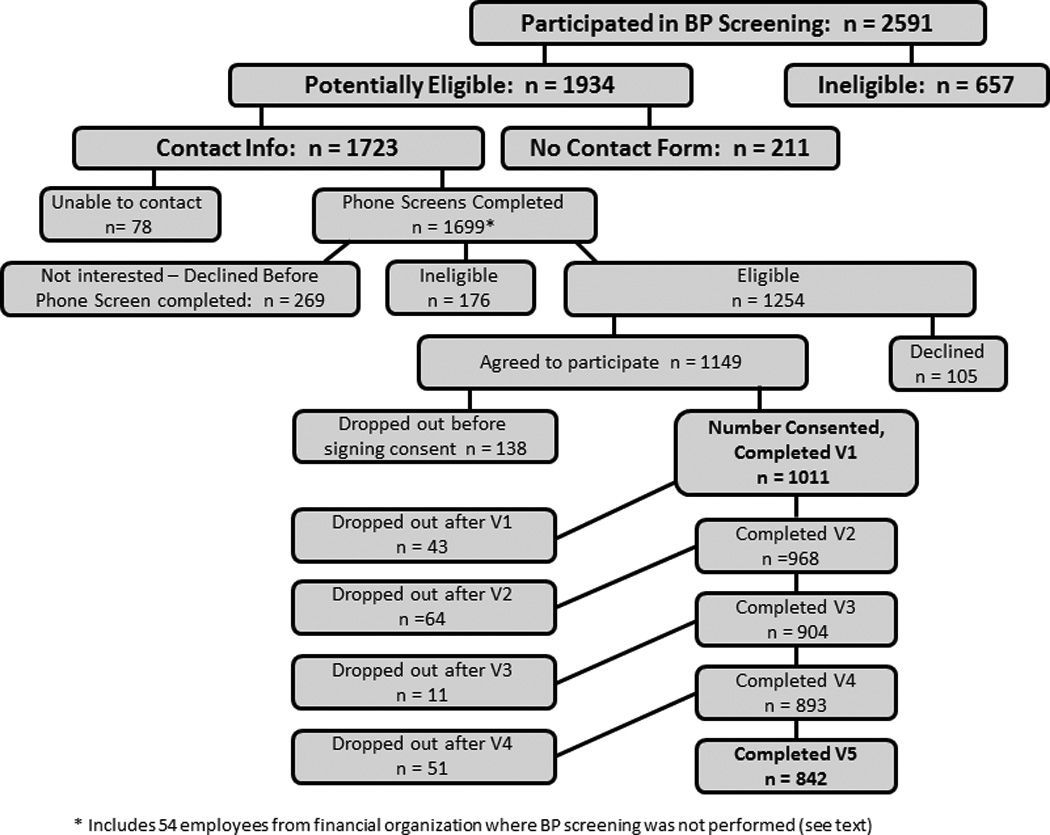
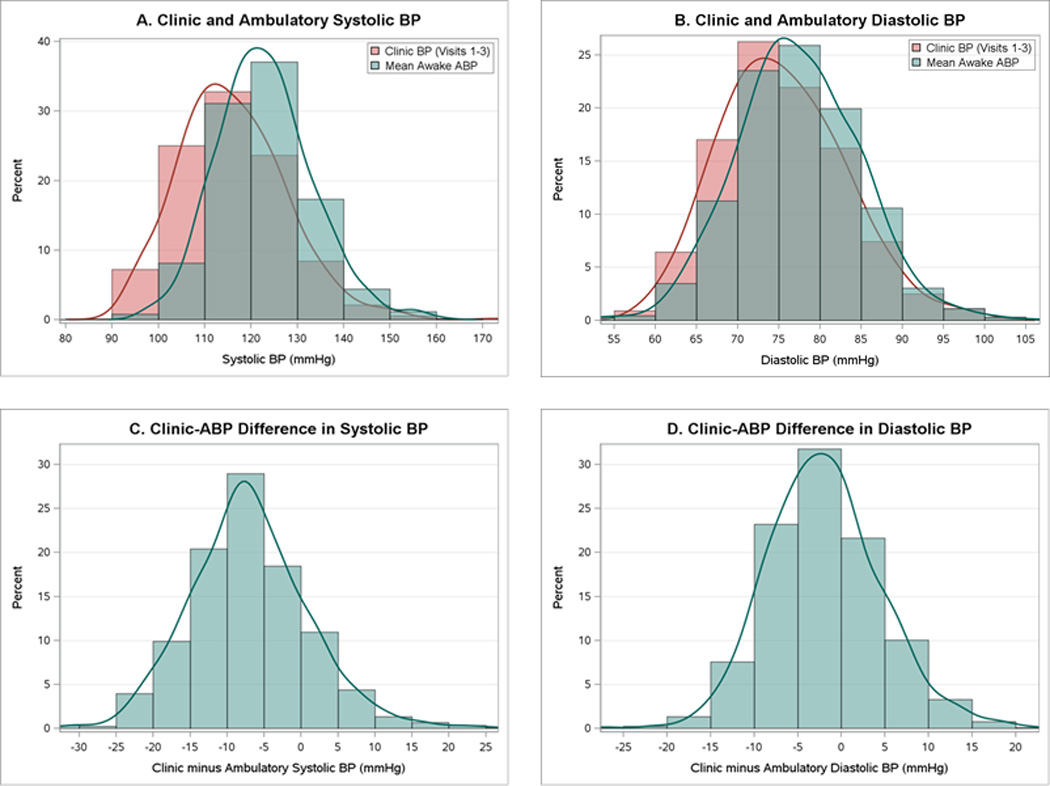
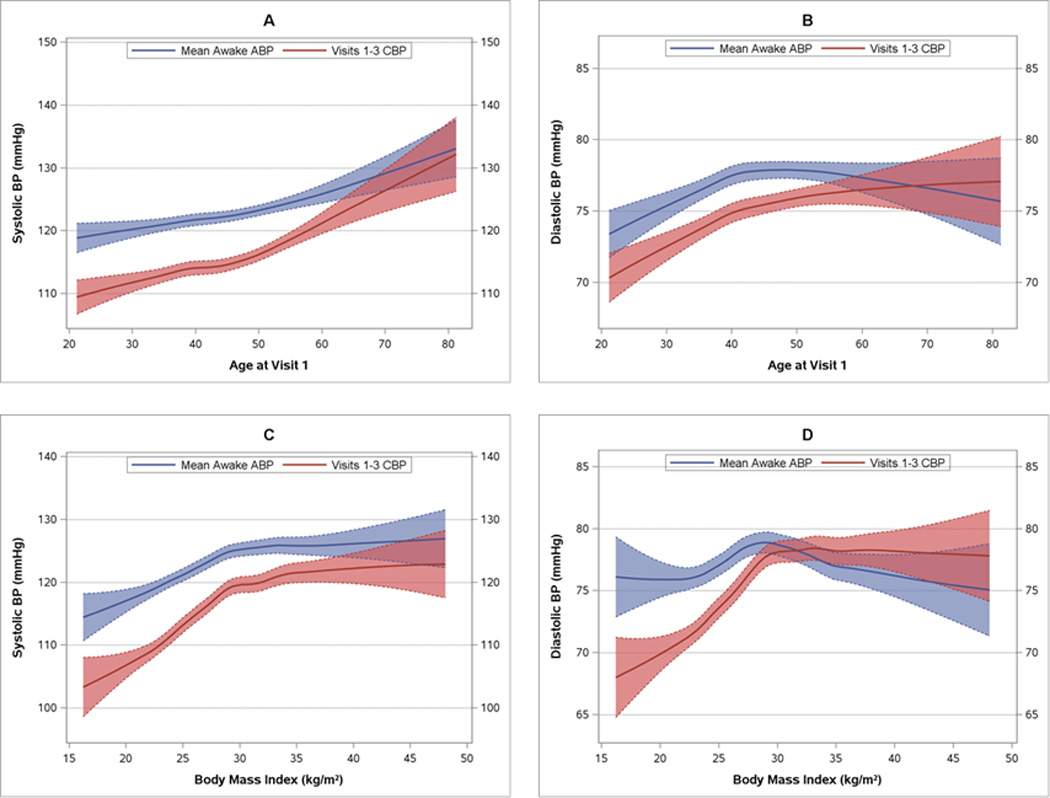
Methods: Between 2005 and 2012, 888 healthy, employed, middle-aged (mean±SD age, 45±10.4 years) individuals (59% female, 7.4% black, 12% Hispanic) with screening BP <160/105 mm Hg and not taking antihypertensive medication completed 3 separate clinic BP assessments and a 24-hour ABP recording for the Masked Hypertension Study. The distributions of CBP, mean awake ABP (aABP), and the CBP-aABP difference in the full sample and by demographic characteristics were compared. Locally weighted scatterplot smoothing was used to model the relationship of the BP measures to age and body mass index. The prevalence of discrepancies in ABP- versus CBP-defined hypertension status-white-coat hypertension and masked hypertension-were also examined.
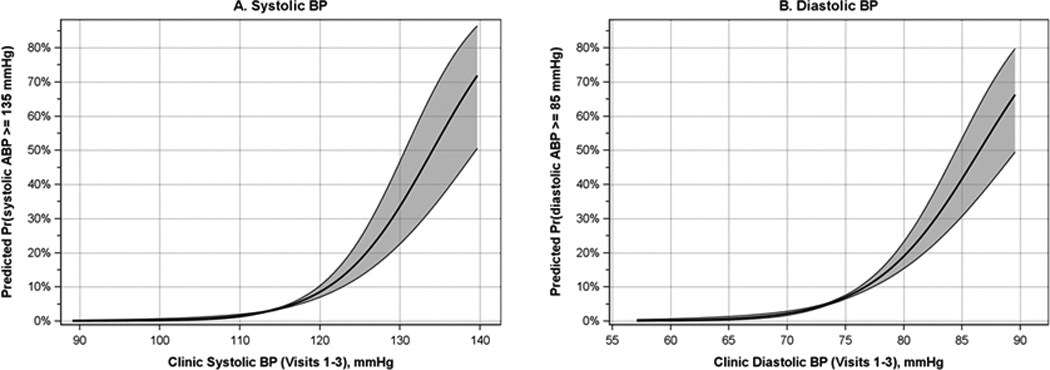
Results: Average systolic/diastolic aABP (123.0/77.4±10.3/7.4 mm Hg) was significantly higher than the average of 9 CBP readings over 3 visits (116.0/75.4±11.6/7.7 mm Hg). aABP exceeded CBP by >10 mm Hg much more frequently than CBP exceeded aABP. The difference (aABP>CBP) was most pronounced in young adults and those with normal body mass index. The systolic difference progressively diminished, but did not disappear, at older ages and higher body mass indexes. The diastolic difference vanished around age 65 and reversed (CBP>aABP) for body mass index >32.5 kg/m2. Whereas 5.3% of participants were hypertensive by CBP, 19.2% were hypertensive by aABP; 15.7% of those with nonelevated CBP had masked hypertension.
Conclusions: Contrary to a widely held belief, based primarily on cohort studies of patients with elevated CBP, ABP is not usually lower than CBP, at least not among healthy, employed individuals. Furthermore, a substantial proportion of otherwise healthy individuals with nonelevated CBP have masked hypertension. Demonstrated CBP-aABP gradients, if confirmed in representative samples (eg, NHANES [National Health and Nutrition Examination Survey]), could provide guidance for primary care physicians as to when, for a given CBP, 24-hour ABP would be useful to identify or rule out masked hypertension.
Keywords: blood pressure; blood pressure monitoring, ambulatory; masked hypertension.
© 2016 American Heart Association, Inc.
Conflict of interest statement
Disclosures: None
Figures
Comment in
-
Time to Abandon Clinic Blood Pressure for the Diagnosis of Hypertension?Circulation. 2016 Dec 6;134(23):1808-1811. doi: 10.1161/CIRCULATIONAHA.116.023914. Circulation. 2016. PMID: 27920073 No abstract available.
Similar articles
-
Masked hypertension assessed by ambulatory blood pressure versus home blood pressure monitoring: is it the same phenomenon?Am J Hypertens. 2005 Jun;18(6):772-8. doi: 10.1016/j.amjhyper.2005.01.003. Am J Hypertens. 2005. PMID: 15925734
-
Prevalence of Masked Hypertension Among US Adults With Nonelevated Clinic Blood Pressure.Am J Epidemiol. 2017 Feb 1;185(3):194-202. doi: 10.1093/aje/kww237. Am J Epidemiol. 2017. PMID: 28100465 Free PMC article.
-
Prevalence of Masked Hypertension and Its Association With Subclinical Cardiovascular Disease in African Americans: Results From the Jackson Heart Study.J Am Heart Assoc. 2016 Mar 29;5(3):e002284. doi: 10.1161/JAHA.115.002284. J Am Heart Assoc. 2016. PMID: 27025968 Free PMC article.
-
Blood Pressure Monitoring. Task force III: Target-organ damage, morbidity and mortality.Blood Press Monit. 1999 Dec;4(6):303-17. doi: 10.1097/00126097-199912000-00004. Blood Press Monit. 1999. PMID: 10602535 Review.
-
The ambulatory blood pressure in normotensive and hypertensive subjects: results from an international database.Neth J Med. 1995 Feb;46(2):106-14. doi: 10.1016/0300-2977(94)00057-g. Neth J Med. 1995. PMID: 7885522 Review.
Cited by
-
Heightened Stress in Employed Individuals Is Linked to Altered Variability and Inertia in Emotions.Front Psychol. 2020 Jun 16;11:1152. doi: 10.3389/fpsyg.2020.01152. eCollection 2020. Front Psychol. 2020. PMID: 32612555 Free PMC article.
-
Role of ambulatory blood pressure monitoring for the management of hypertension in Asian populations.J Clin Hypertens (Greenwich). 2017 Dec;19(12):1240-1245. doi: 10.1111/jch.13086. Epub 2017 Aug 22. J Clin Hypertens (Greenwich). 2017. PMID: 28834205 Free PMC article. Review.
-
Development of Predictive Equations for Nocturnal Hypertension and Nondipping Systolic Blood Pressure.J Am Heart Assoc. 2020 Jan 21;9(2):e013696. doi: 10.1161/JAHA.119.013696. Epub 2020 Jan 9. J Am Heart Assoc. 2020. PMID: 31914878 Free PMC article.
-
Reallocations of Time Between Sleep, Sedentary Behavior, and Physical Activity and Their Associations With 24-Hour Blood Pressure.Am J Hypertens. 2025 Feb 18;38(3):164-167. doi: 10.1093/ajh/hpae149. Am J Hypertens. 2025. PMID: 39607720
-
Impact of Asleep and 24-Hour Blood Pressure Data on the Prevalence of Masked Hypertension by Race/Ethnicity.Am J Hypertens. 2022 Jul 1;35(7):627-637. doi: 10.1093/ajh/hpac027. Am J Hypertens. 2022. PMID: 35303061 Free PMC article.
References
-
- Perloff D, Sokolow M, Cowan R. The prognostic value of ambulatory blood pressures. JAMA. 1983;249:2792–2798. - PubMed
-
- Piper MA, Evans CV, Burda BU, Margolis KL, O’Connor E, Smith N, Webber E, Perdue LA, Bigler KD, Whitlock EP. Screening for High Blood Pressure in Adults: A Systematic Evidence Review for the US Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality (US); 2014. U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews. - PubMed
-
- Conen D, Bamberg F. Noninvasive 24-h ambulatory blood pressure and cardiovascular disease: a systematic review and meta-analysis. J Hypertens. 2008;26:1290–1299. - PubMed
-
- Siu AL. Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;163:778–786. - PubMed
-
- Pickering TG, James GD, Boddie C, Harshfield GA, Blank S, Laragh JH. How common is white coat hypertension? JAMA. 1988;259:225–228. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
