

Review
doi: 10.1212/WNL.0000000000003414.
NMDA receptor encephalitis and other antibody-mediated disorders of the synapse: The 2016 Cotzias Lecture
Affiliations
- PMID: 27920282
- PMCID: PMC5177671
- DOI: 10.1212/WNL.0000000000003414
Item in Clipboard
Review
NMDA receptor encephalitis and other antibody-mediated disorders of the synapse: The 2016 Cotzias Lecture
Neurology.
.
Abstract
Investigations during the last 10 years have revealed a group of disorders mediated by antibodies against ion channels and synaptic receptors, which cause both neurologic and psychiatric symptoms. In this review, I discuss the process of discovery and immunologic triggers of these disorders, and use anti-NMDA receptor encephalitis to emphasize the importance of understanding the underlying physiopathologic mechanisms in those diseases. A better knowledge of these mechanisms reveals points of convergence with other disorders (e.g., schizophrenia), suggests treatment strategies beyond immunotherapy, and is helping us understand how memories are formed and retrieved.
© 2016 American Academy of Neurology.
Figures
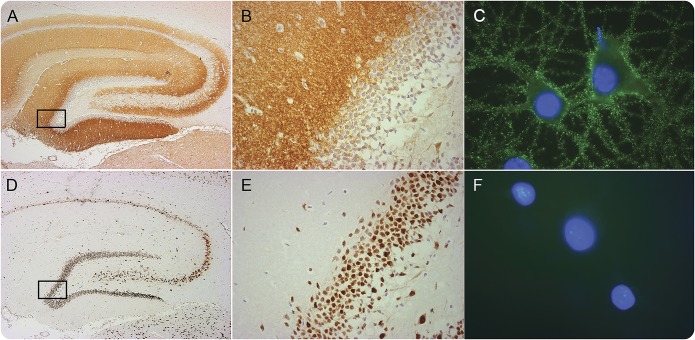
Section of rat hippocampus immunostained with an autoantibody against a synaptic NMDA receptor (NMDAR) from a patient with anti-NMDAR encephalitis (A, B) compared with the reactivity of an autoantibody against an intracellular neuronal protein (Hu) from a patient with paraneoplastic encephalitis (D, E). The boxed areas are shown in detail in (B) and (E). The demonstration that the target antigen is on the neuronal cell surface is provided by immunocytochemistry with live neurons (obtained from dissociated rat hippocampus): the NMDAR antibodies show intense reactivity with the cognate receptor on the cell surface (C) whereas the Hu antibodies do not show reactivity because they do not reach the intracellular target (F). Scale bars: A, B = 500 μm; C, D = 20 μm; E, F = 10 μm. Adapted from Lancaster et al., with permission.
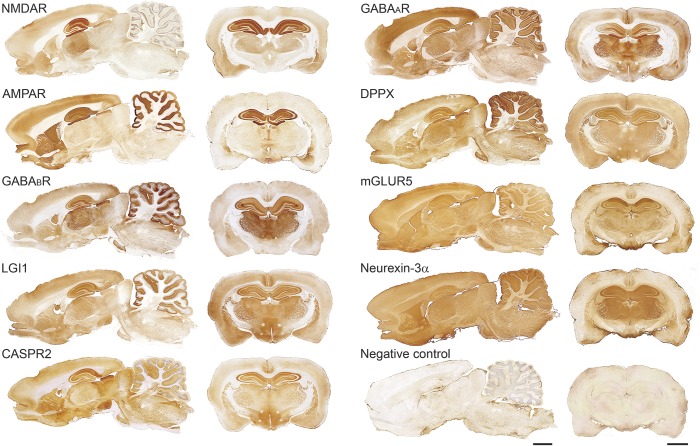
Sagittal and coronal sections of rat brain immunostained with 9 different autoantibodies from patients with different types of autoimmune encephalitis. For each antibody, the pattern of neuropil immunostaining is highly suggestive that the antigen is on the neuronal cell surface (figure 1). Scale bars: all panels = 2 mm. AMPAR = α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor; CASPR2 = contactin-associated protein-like 2; DPPX = dipeptidyl-peptidase–like protein-6; GABA = γ-aminobutyric acid; LGI1 = leucine-rich glioma inactivated 1; mGluR = metabotropic glutamate receptor; NMDAR = NMDA receptor.
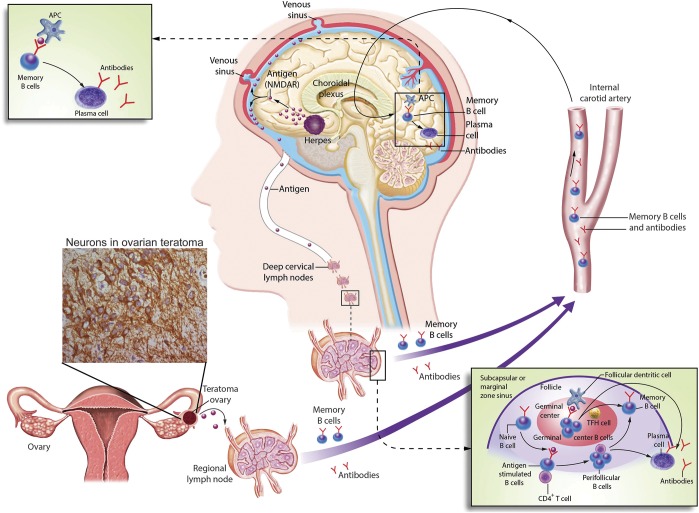
The figure describes 2 known immunologic triggers of anti-NMDAR encephalitis: a tumor (usually ovarian teratoma) and herpes simplex encephalitis. The underlying multistep process between either of these triggers and the CNS production of antibodies is unknown, but the latter has been confirmed in studies demonstrating intrathecal synthesis of antibodies and CNS plasma cells. It is postulated that NMDAR expressed in nervous tissue contained in the tumor, or released by viral-induced neuronal destruction, is either in soluble form or loaded in antigen-presenting cells transported to the regional lymph nodes (e.g., pelvic-abdominal in case of ovarian teratoma or deep cervical lymph nodes in case of herpes encephalitis) where it is presented to the immunologic system. Naive B cells exposed to NMDAR by antigen-presenting cells, and with cooperation of CD4+ T cells, become antigen-experienced memory B cells, differentiating into antibody-producing plasma cells. Memory B cells reach the brain crossing the BBB or the choroidal plexus. In the brain, these B cells undergo restimulation, antigen-driven affinity maturation, clonal expansion, and differentiation into antibody-producing plasma cells. Of note, in approximately 50% of the patients the immunologic trigger of the disease is unknown. The model of tumor as a trigger of autoimmune encephalitis would be similar for other types of encephalitis (table); in tumors other than teratoma (e.g., without nervous tissue within the tumor itself), the antigen is aberrantly expressed by the neoplastic cells. APC = antigen-presenting cell; TFH = follicular helper T cell.
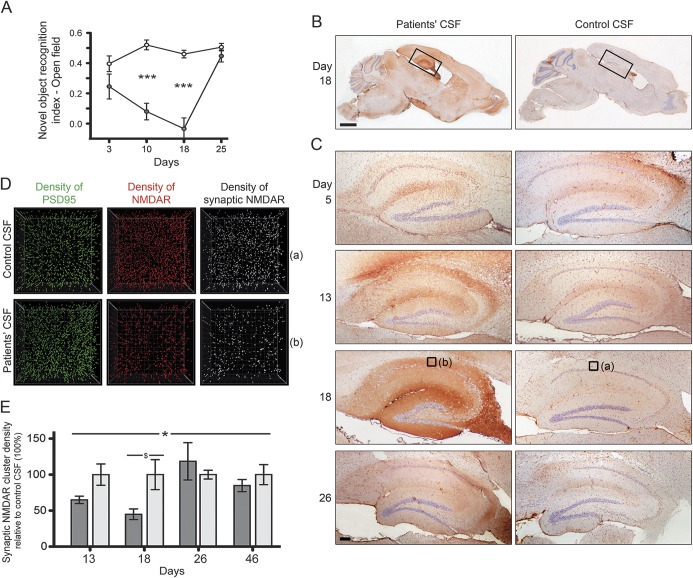
Mice underwent placement of bilateral ventricular catheters connected to subcutaneous osmotic pumps that during 14 days infused CSF from patients with NMDAR antibodies or control CSF. At several timepoints during and after the infusion, animals underwent behavioral testing or were killed to determine the binding and effects of the antibodies. (A) Animals infused with patients' CSF antibodies developed severe memory impairment demonstrated by the novel object recognition test (gray circles, n = 8 mice) compared with animals infused with control CSF (white circles, n = 10 mice). Data presented as standard error of the mean. Significance assessed by 2-way analysis of variance with α-error of 0.05 and post hoc testing with Sidak-Holm adjustment, ***p < 0.001. This memory deficit along with anhedonia-like behavior (not shown here) were accompanied by a progressive accumulation of brain-bound NMDAR antibodies (predominantly in the hippocampus) that was maximal on day 18 (B, C). Quantitative analysis of the NMDAR clusters in 15 areas of the hippocampus (only 1 per brain is shown in [D], which correspond to the small squares [a] and [b] in [C], day 18) demonstrates a significant reduction of density of total cell-surface NMDAR clusters and synaptic NMDAR clusters (defined by colocalization with PSD95) in animals infused with patients' CSF antibodies (D). (E) Quantitative analysis of synaptic NMDAR cluster density in the 2 groups of animals (dark gray: infused with patients' CSF; light gray: infused with control CSF; 5 animals per group). Data presented as standard error of the mean. Significance assessed by 2-way analysis of variance with α-error of 0.05 (*) and post hoc testing with Sidak-Holm adjustment ($), *$p < 0.05. Note that all antibody effects including memory deficits, accumulation of brain-bound human NMDAR antibodies, and reduction of levels of NMDAR became maximal on day 18, and gradually recovered 10 days after stopping the antibody infusion. Scale bars: B = 2 mm; C = 200 μm. Reproduced from Planagumà et al. with permission.
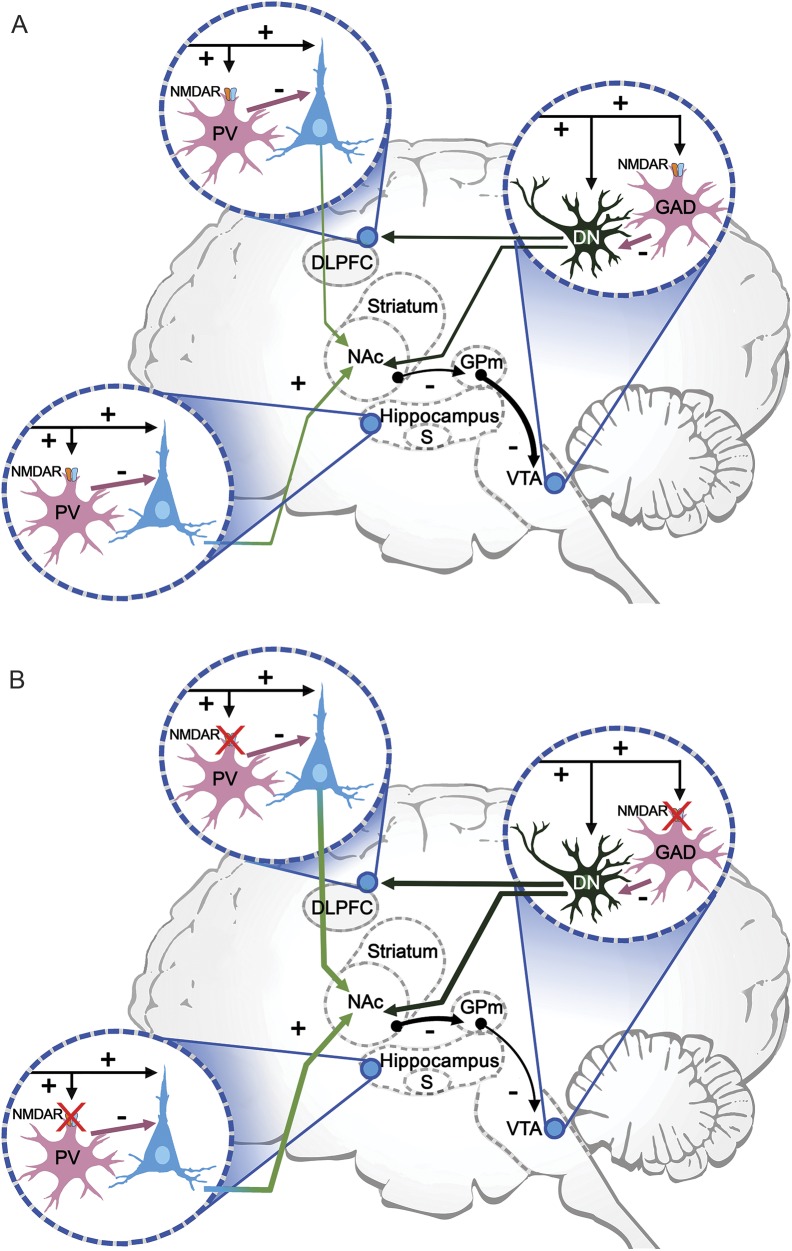
This simplified diagram shows some of the cognitive networks that are affected by NMDAR hypofunction. There are 3 critical nodes: (1) the subiculum, effector region of the hippocampus; (2) the dorsolateral prefrontal cortex (DLPFC), which supports executive function and working memory; and (3) the ventral tegmental area (VTA), which facilitates episodic and working memory, and motivation. (A) At each of these nodes, glutamatergic excitatory inputs (mainly from lateral hypothalamus) to pyramidal or dopaminergic neurons provide collaterals to NMDAR-bearing GABAergic interneurons, which in turn inhibit excessive pyramidal firing. GABAergic interneurons in the subiculum and DLPFC are parvalbumin positive (PV), and in the DLPFC are characterized as the fast-spiking cells, which are involved in the generation of synchronous gamma oscillations. In the VTA, GABAergic interneurons also contain NMDAR and are glutamic acid decarboxylase (GAD)–positive. Dopaminergic VTA neurons (DN) project to the nucleus accumbens (NAc), DLPFC, and hippocampus (not shown). The NAc inhibits the globus pallidus medialis (GPm), which in turn tonically inhibits VTA dopaminergic neurons. (B) NMDAR hypofunction (one of the leading theories of schizophrenia) is associated with increased pyramidal firing, which increases the inhibitory activity of the NAc over the GPm and lessens the inhibitory tone over the VTA dopaminergic neurons. This leads to an increased production of dopamine, as found in psychoses, along with impaired working memory related to the altered function of PV interneurons (adapted from Masdeu et al., with permission).
References
-
- Drachman DB, Adams RN, Josifek LF, Self SG. Functional activities of autoantibodies to acetylcholine receptors and the clinical severity of myasthenia gravis. N Engl J Med 1982;307:769–775. - PubMed
-
- Darnell RB, Posner JB. Paraneoplastic syndromes involving the nervous system. N Engl J Med 2003;349:1543–1554. - PubMed
-
- Vora NM, Holman RC, Mehal JM, Steiner CA, Blanton J, Sejvar J. Burden of encephalitis-associated hospitalizations in the United States, 1998-2010. Neurology 2014;82:443–451. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources