

Neoadjuvant Chemotherapy with Docetaxel, Carboplatin and Weekly Trastuzumab Is Active in HER2-Positive Early Breast Cancer: Results after a Median Follow-Up of over 4 Years
- PMID: 27920624
- PMCID: PMC5123029
- DOI: 10.1159/000452079
Neoadjuvant Chemotherapy with Docetaxel, Carboplatin and Weekly Trastuzumab Is Active in HER2-Positive Early Breast Cancer: Results after a Median Follow-Up of over 4 Years
Abstract
Introduction: Most patients with HER2-positive breast cancer receive chemotherapy and trastuzumab. Data from adjuvant trials have shown that the combination of docetaxel, carboplatin and weekly trastuzumab (TCH) is well tolerated and as effective as anthracycline-containing regimes. Previous investigations on neoadjuvant treatment with taxanes, platinum salts and trastuzumab showed pathological complete remission (pCR) rates between 43.3 and 76%. To date, the longest published follow-up in this indication is 3 years. Here we present 4-year follow-up data for a cohort of 78 patients treated with neoadjuvant TCH.
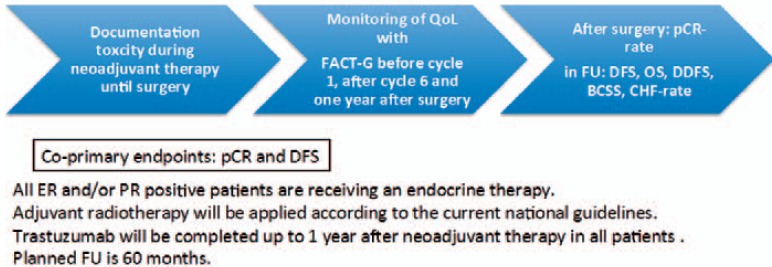
Methods: Between 2009 and 2014 we treated 78 patients with operable HER2-positive breast cancer with a neoadjuvant schedule of docetaxel (75 mg/m2) and carboplatin (AUC 6) every 3 weeks (q3w) and trastuzumab (4 mg/kg loading dose then 2 mg/kg) q1w. Lymph node involvement was verified by sentinel lymph node or core-cut biopsy. Patients were diagnosed at a mean age of 55.5 years; 65.4% had hormone receptor-positive tumors, 34.6% presented with grade 3 disease and 51.3% of patients were node positive. Patients were monitored every 2 cycles by ultrasound. After 6 cycles of chemotherapy all patients had surgery. Axillary dissection was performed in case of positive lymph node status prior to TCH. After surgery, trastuzumab was continued q3w up to 1 year.
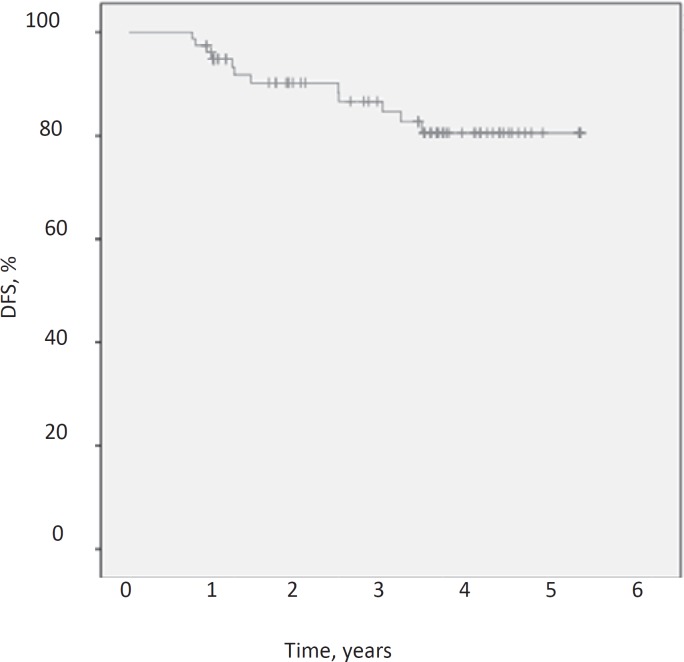
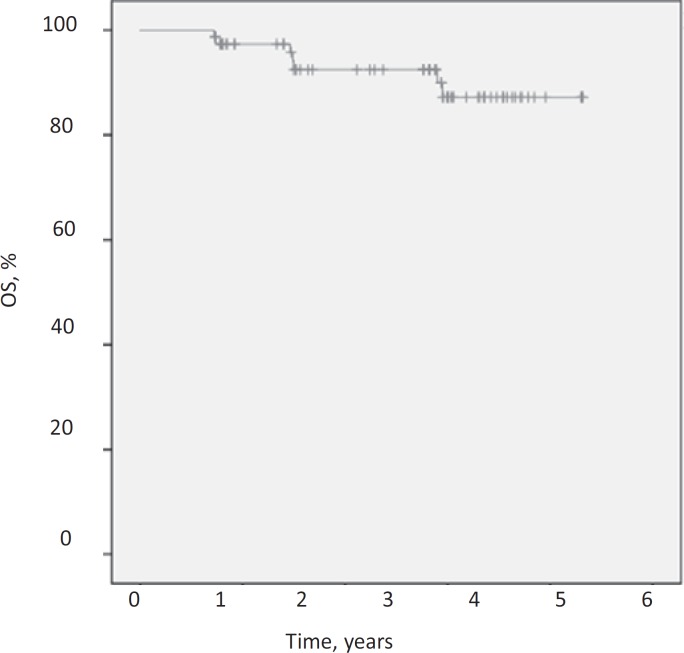
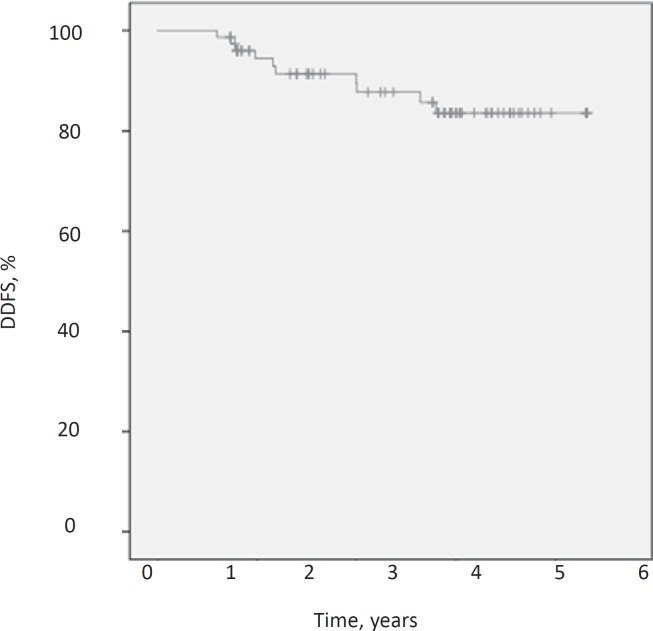
Results: No grade III/IV toxicities occurred and no case of congestive heart failure was observed. Neither dose modifications nor dose delays were necessary. 34 of the 78 patients (43.6%) achieved a pCR, 27 of the 40 node-positive patients (67.5%) experienced nodal conversion. After a median follow up of 48.5 months the disease-free survival (DFS) was 84.6%, the distant disease-free survival (DDFS) was 87.2% and the overall survival (OS) was 91%. Only T stage and nodal status at baseline were found to be significantly associated with survival estimates.
Conclusion: The anthracycline-free regimen TCH is effective and safe in the neoadjuvant therapy of HER2-positive breast cancer, yielding DFS, DDFS and OS probabilities comparable to the results of adjuvant trials. Our data support the use of TCH as a neoadjuvant therapy regimen for patients with HER2-positive breast cancer. They also strongly encourage the use of taxanes and platinum salts as the chemotherapy backbone in studies investigating dual blockade with trastuzumab and pertuzumab in the neoadjuvant setting.
Keywords: Anthracycline free; Breast cancer; HER2 positive; Neoadjuvant therapy; TCH.
Figures
References
-
- Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659–1672. - PubMed
-
- Untch M, Rezai M, Loibl S, et al. Neoadjuvant treatment with trastuzumab in HER2-positive breast cancer: results from the GeparQuattro study. J Clin Oncol. 2010;28:2024–2031. - PubMed
-
- Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet. 2014;384:164–172. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
