

Trends and determinant factors in the use of cardiac resynchronization therapy devices in Japan: Analysis of the Japan cardiac device treatment registry database
- PMID: 27920834
- PMCID: PMC5129119
- DOI: 10.1016/j.joa.2016.04.002
Trends and determinant factors in the use of cardiac resynchronization therapy devices in Japan: Analysis of the Japan cardiac device treatment registry database
Abstract
Background: The choice of cardiac resynchronization therapy device, with (CRT-D) or without (CRT-P) a defibrillator, in patients with heart failure largely depends on the physician׳s discretion, because it has not been established which subjects benefit most from a defibrillator.
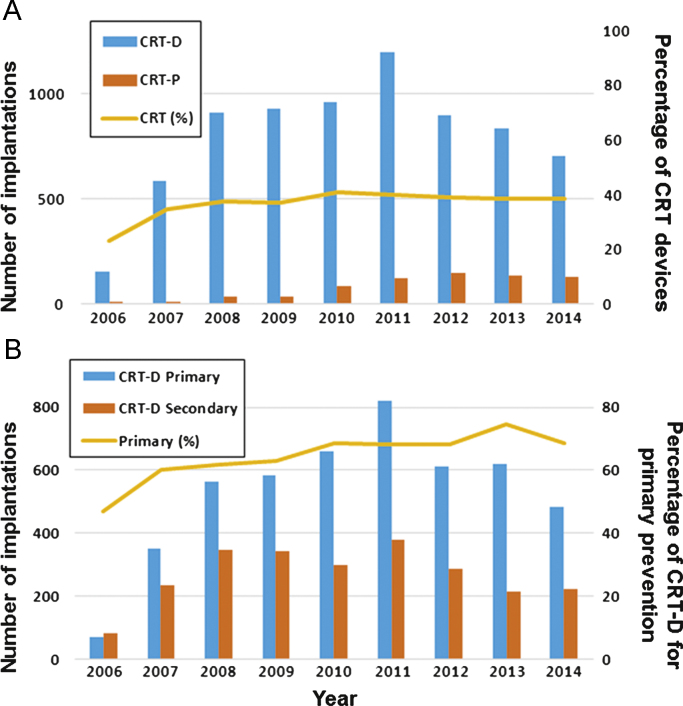
Methods: We examined the annual trend of CRT device implantations between 2006 and 2014, and evaluated the factors related to the device selection (CRT-D or CRT-P) for primary prevention of sudden cardiac death in patients with heart failure by analyzing the Japan Cardiac Device Treatment Registry (JCDTR) database from January 2011 and August 2015 (CRT-D, n=2714; CRT-P, n=555).
Results: The proportion of CRT-D implantations for primary prevention among all the CRT-D recipients was more than 70% during the study period. The number of CRT-D implantations for primary prevention reached a maximum in 2011 and decreased gradually between 2011 and 2014, whereas CRT-P implantations increased year by year until 2011 and remained unchanged in recent years. Multivariate analysis identified age (odds ratio [OR] 0.92, 95% confidence interval [CI] 0.90-0.95, P<0.0001), male sex (OR 1.99, 95% CI 1.28-3.11, P<0.005), reduced left ventricular ejection fraction (LVEF) (OR 0.96, 95% CI 0.94-0.98, P<0.0001), and non-sustained ventricular tachycardia (NSVT) (OR 2.85, 95% CI 1.87-4.35, P<0.0001) as independent factors favoring the choice of CRT-D.
Conclusions: Younger age, male sex, reduced LVEF, and a history of NSVT were independently associated with the choice of CRT-D for primary prevention of sudden cardiac death in patients with heart failure in Japan.
Keywords: Cardiac resynchronization therapy; Defibrillator; Heart failure; Primary prevention.
Figures

Similar articles
-
Prognostic significance of nonsustained ventricular tachycardia in patients receiving cardiac resynchronization therapy for primary prevention: Analysis of the Japan cardiac device treatment registry database.J Arrhythm. 2018 Jan 12;34(2):139-147. doi: 10.1002/joa3.12023. eCollection 2018 Apr. J Arrhythm. 2018. PMID: 29657589 Free PMC article.
-
Cardiac resynchronization therapy with a defibrillator in non-ischemic and ischemic patients for primary and secondary prevention of sudden cardiac death: Analysis of the Japan cardiac device treatment registry database.J Arrhythm. 2023 Aug 24;39(5):757-765. doi: 10.1002/joa3.12916. eCollection 2023 Oct. J Arrhythm. 2023. PMID: 37799798 Free PMC article.
-
Survival and Heart Failure Hospitalization in Patients With Cardiac Resynchronization Therapy With or Without a Defibrillator for Primary Prevention in Japan - Analysis of the Japan Cardiac Device Treatment Registry Database.Circ J. 2017 Nov 24;81(12):1798-1806. doi: 10.1253/circj.CJ-17-0234. Epub 2017 Jun 13. Circ J. 2017. PMID: 28626201
-
Long-term efficacy of implantable cardiac resynchronization therapy plus defibrillator for primary prevention of sudden cardiac death in patients with mild heart failure: an updated meta-analysis.Heart Fail Rev. 2016 Jul;21(4):447-53. doi: 10.1007/s10741-016-9550-y. Heart Fail Rev. 2016. PMID: 27043219 Review.
-
Cause-of-death analysis in patients with cardiac resynchronization therapy with or without a defibrillator: a systematic review and proportional meta-analysis.Europace. 2018 Mar 1;20(3):481-491. doi: 10.1093/europace/eux094. Europace. 2018. PMID: 28666319
Cited by
-
Improved outcomes of cardiac resynchronization therapy with a defibrillator in systolic heart failure: Analysis of the Japan cardiac device treatment registry database.J Arrhythm. 2023 Nov 14;40(1):30-37. doi: 10.1002/joa3.12952. eCollection 2024 Feb. J Arrhythm. 2023. PMID: 38333398 Free PMC article.
-
Utilization and Efficacy of Cardiac Resynchronization Therapy in Patients With Chronic Heart Failure - A Report From the CHART-2 Study.Circ Rep. 2022 May 25;4(6):264-273. doi: 10.1253/circrep.CR-22-0036. eCollection 2022 Jun 10. Circ Rep. 2022. PMID: 35774073 Free PMC article.
-
A Predictive Model for Super-Response to Cardiac Resynchronization Therapy: The QQ-LAE Score.Cardiol Res Pract. 2020 Aug 28;2020:3856294. doi: 10.1155/2020/3856294. eCollection 2020. Cardiol Res Pract. 2020. PMID: 32908692 Free PMC article.
-
Prognostic significance of nonsustained ventricular tachycardia in patients receiving cardiac resynchronization therapy for primary prevention: Analysis of the Japan cardiac device treatment registry database.J Arrhythm. 2018 Jan 12;34(2):139-147. doi: 10.1002/joa3.12023. eCollection 2018 Apr. J Arrhythm. 2018. PMID: 29657589 Free PMC article.
-
The use of angiotensin II receptor blocker is associated with greater recovery of cardiac function than angiotensin-converting enzyme inhibitor in dilated cardiomyopathy.ESC Heart Fail. 2022 Apr;9(2):1175-1185. doi: 10.1002/ehf2.13790. Epub 2022 Feb 8. ESC Heart Fail. 2022. PMID: 35137537 Free PMC article.
References
-
- Abraham W.T., Fisher W.G., Smith A.L. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002;346:1845–1853. - PubMed
-
- Bristow M.R., Saxon L.A., Boehmer J. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140–2150. - PubMed
-
- Cleland J.G., Daubert J.C., Erdmann E. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–1549. - PubMed
-
- Goldenberg I., Kutyifa V., Klein H.U. Survival with cardiac-resynchronization therapy in mild heart failure. N Engl J Med. 2014;370:1694–1701. - PubMed
-
- Moss A.J., Hall W.J., Cannom D.S. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009;361:1329–1338. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
