

Choledochoduodenal fistula in the setting of Crohn's disease
- PMID: 27920850
- PMCID: PMC5128396
- DOI: 10.1016/j.radcr.2016.08.018
Choledochoduodenal fistula in the setting of Crohn's disease
Abstract
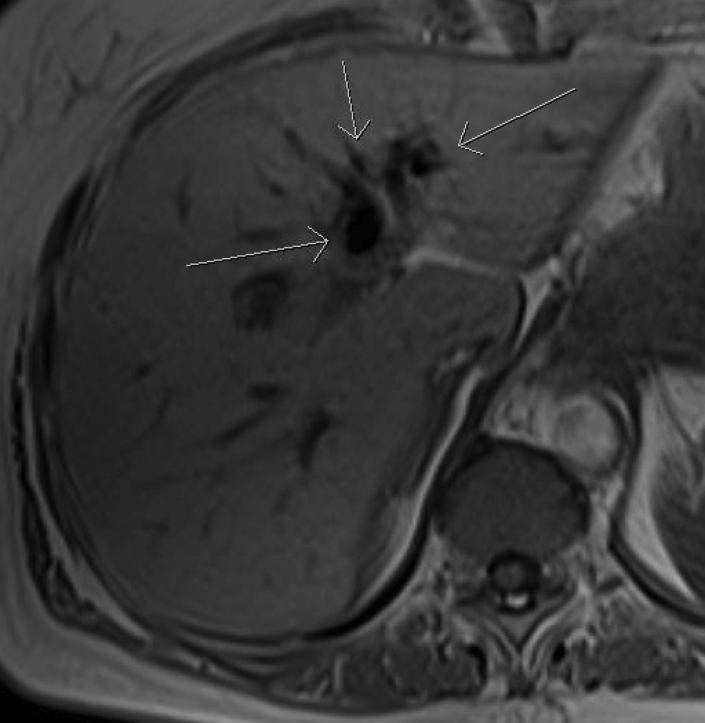
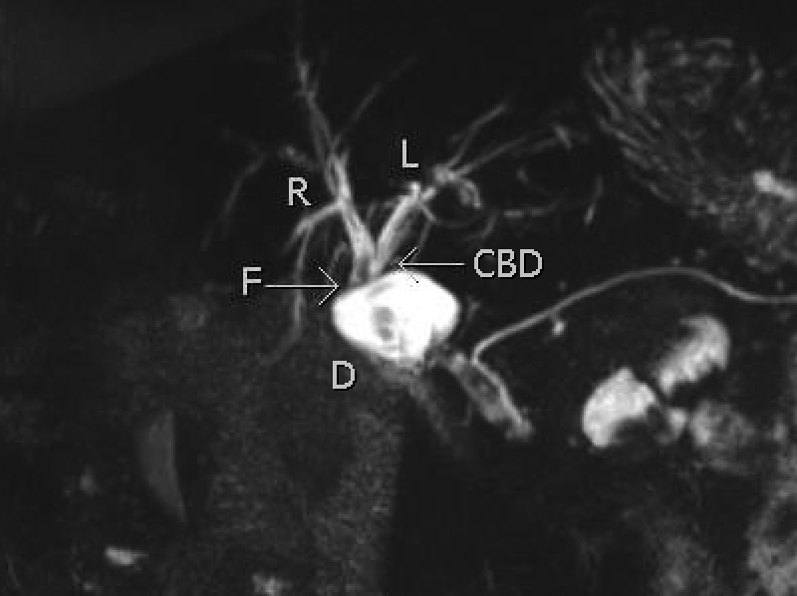
Of all the spontaneous fistulas that occur between the extrahepatic biliary system and the intestine, a choledochoduodenal fistula is rarely seen. When it does occur, it is most often secondary to a perforated duodenal ulcer, choledocholithiasis, or cholelithiasis. It may also be seen following complications related to iatrogenic injury or tuberculosis. Generally, choledochoduodenal fistulas are asymptomatic, but may present with vague abdominal pain, fever, and other symptoms related to cholangitis. As a result, they can be difficult to diagnose clinically before imaging is obtained. We present a case of a 74 year old, asymptomatic, female with a past medical history significant for Crohn's disease who was found to have a choledochoduodenal fistula demonstrated on MRCP, possibly secondary to her underlying inflammatory bowel disease.
Keywords: Bilioenteric fistula; Choledochoduodenal fistula; Crohn's disease.
Figures



References
-
- Jordan P., Stirrett L. Treatment of spontaneous internal biliary fistula caused by duodenal ulcer. Am J Surg. 1956;91(3):307–313. - PubMed
-
- Page J., Dow J., Dundas D. Ulcerogenic choledochoduodenal fistula. Clin Radiol. 1989;40(1):58–60. - PubMed
-
- Leblanc K., Barr L., Rush B. Spontaneous biliary enteric fistulas. South Med J. 1983;76(10):1249–1252. - PubMed
-
- Aziz M., Ahmed M., Siddiqui M., Shipa M., Sarker S., Arif S. Choledochoduodenal fistula secondary to duodenal ulcer disease and choledocholithiasis: report of 2 cases. J Armed Forces Med Coll, Bangladesh. 2008;4(2):38–41.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
