

Peripheral Stent Thrombosis Leading to Acute Limb Ischemia and Major Amputation: Incidence and Risk Factors in the Aortoiliac and Femoropopliteal Arteries
- PMID: 27921154
- PMCID: PMC5288432
- DOI: 10.1007/s00270-016-1513-0
Peripheral Stent Thrombosis Leading to Acute Limb Ischemia and Major Amputation: Incidence and Risk Factors in the Aortoiliac and Femoropopliteal Arteries
Abstract
Purpose: To report the real-world incidence and risk factors of stent thrombosis in the aortoiliac and femoropopliteal arteries in case of bare nitinol stent (BNS) or covered nitinol stent (CNS) placement from a single-centre retrospective audit.
Materials and methods: Medical records of consecutive patients treated with peripheral stent placement for claudication or critical limb ischemia were audited for definite stent thrombosis defined as imaging confirmed stent thrombosis that presented as acute limb-threatening ischemia. Cases were stratified between aortoiliac and femoropopliteal anatomy. Cox regression analysis was employed to adjust for baseline clinical and procedural confounders and identify predictors of stent thrombosis and major limb loss.
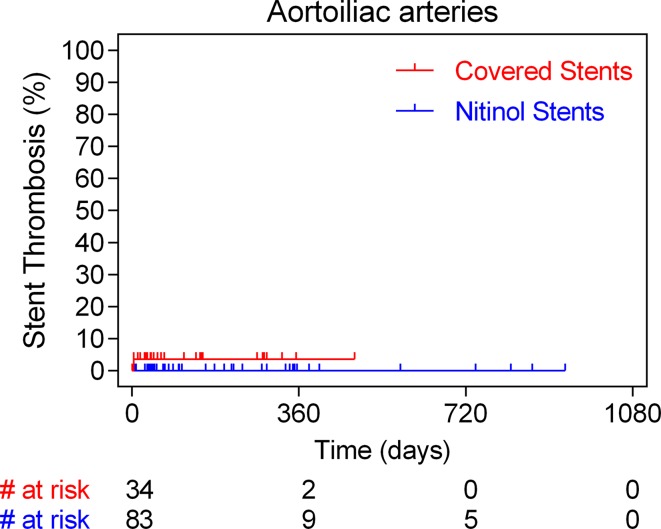
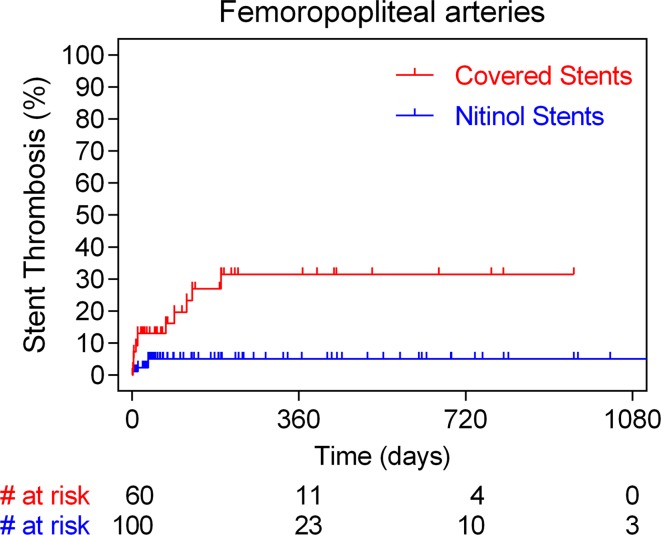
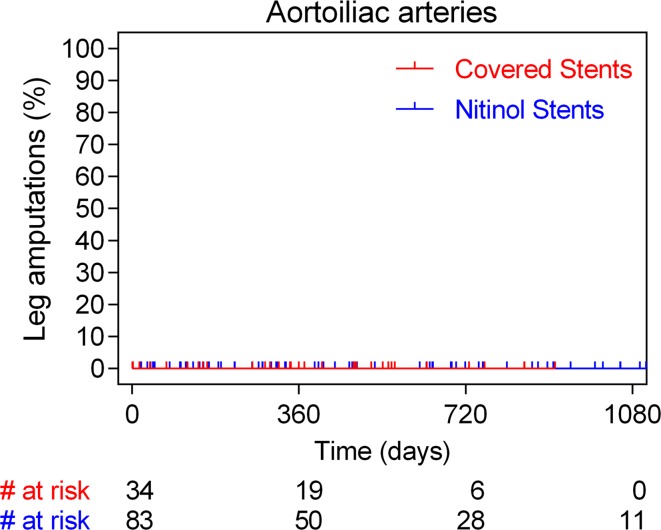
Results: 256 patients (n = 277 limbs) were analysed over a 5-year period (2009-2014) including 117 aortoiliac stents (34 CNS; 12.8 ± 5.0 cm and 83 BNS; 7.8 ± 4.0 cm) and 160 femoropopliteal ones (60 CNS; 21.1 ± 11.0 cm and 100 BNS; 17.5 ± 11.9 cm). Median follow-up was 1 year. Overall stent thrombosis rate was 6.1% (17/277) after a median of 43 days (range 2-192 days) and affected almost exclusively the femoropopliteal segment (12/60 in the CNS cohort vs. 4/100 in the BNS; p = 0.001). Annualized stent thrombosis rates (per 100 person-years) were 12.5% in case of CNS and 1.4% in case of BNS (HR 6.3, 95% CI 2.4-17.9; p = 0.0002). Corresponding major amputations rates were 8.7 and 2.5%, respectively (HR 4.5, 95% CI 2.7-27.9; p = 0.0006). On multivariable analysis, critical leg ischemia and CNS placement were the only predictors of stent thrombosis. Diabetes, critical leg ischemia, femoropopliteal anatomy, long stents and CNS were independent predictors of major amputations.
Conclusions: Placement of long femoropopliteal covered nitinol stents is associated with an increased incidence of acute stent thrombosis and ensuing major amputation. Risks are significantly lower in the aortoiliac vessels and with use of bare nitinol stents.
Keywords: Acute limb ischemia; Covered stent; Major amputation; Nitinol stent; Stent thrombosis.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest. Ethical approval This was a retrospective clinical audit. For this type of study, formal consent is not required.
Figures

References
-
- Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Associations for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (writing committee to develop guidelines for the management of patients with peripheral arterial disease)–summary of recommendations. J Vasc Interv Radiol. 2006;17(9):1383–1397. doi: 10.1097/01.RVI.0000240426.53079.46. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
