

Percutaneous Gastrostomy Device for the Treatment of Class II and Class III Obesity: Results of a Randomized Controlled Trial
- PMID: 27922026
- PMCID: PMC5350543
- DOI: 10.1038/ajg.2016.500
Percutaneous Gastrostomy Device for the Treatment of Class II and Class III Obesity: Results of a Randomized Controlled Trial
Abstract
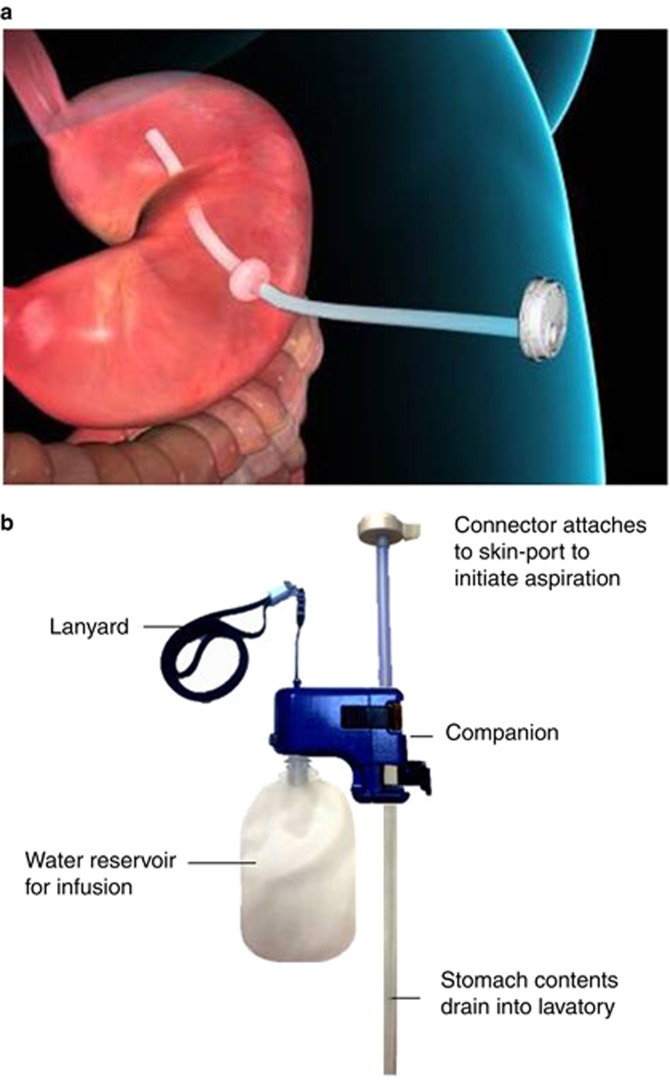
Objectives: The AspireAssist System (AspireAssist) is an endoscopic weight loss device that is comprised of an endoscopically placed percutaneous gastrostomy tube and an external device to facilitate drainage of about 30% of the calories consumed in a meal, in conjunction with lifestyle (diet and exercise) counseling.
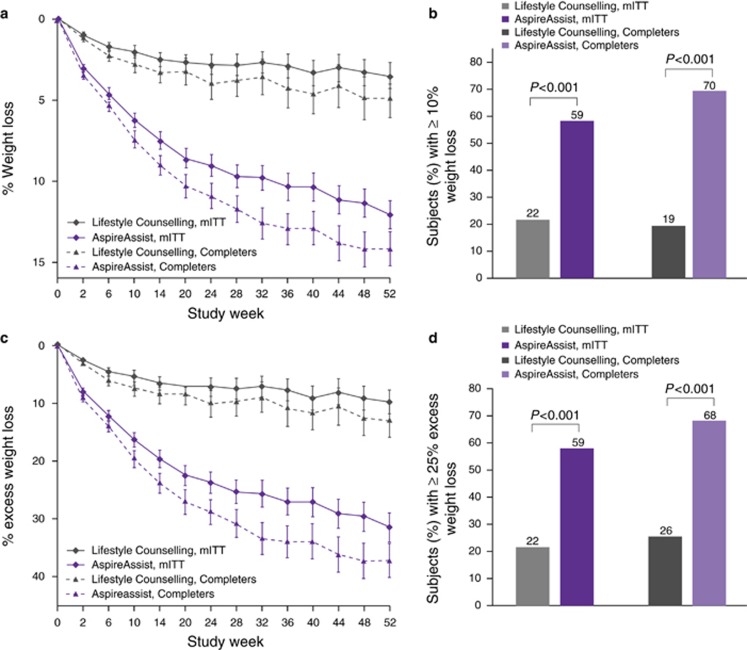
Methods: In this 52-week clinical trial, 207 participants with a body-mass index (BMI) of 35.0-55.0 kg/m2 were randomly assigned in a 2:1 ratio to treatment with AspireAssist plus Lifestyle Counseling (n=137; mean BMI was 42.2±5.1 kg/m2) or Lifestyle Counseling alone (n=70; mean BMI was 40.9±3.9 kg/m2). The co-primary end points were mean percent excess weight loss and the proportion of participants who achieved at least a 25% excess weight loss.
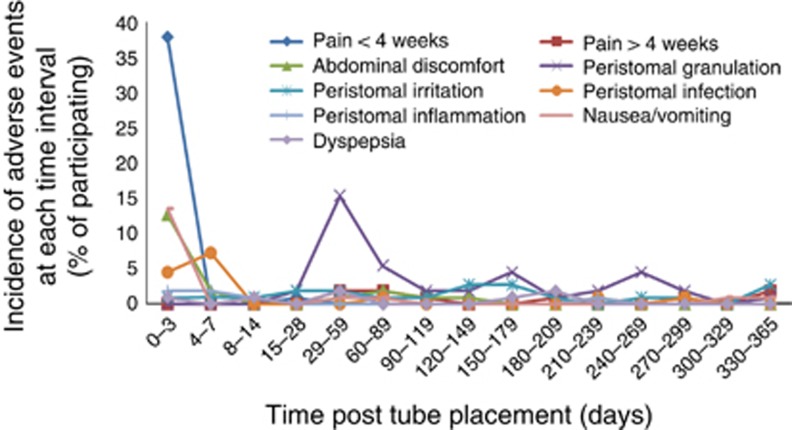
Results: At 52 weeks, participants in the AspireAssist group, on a modified intent-to-treat basis, had lost a mean (±s.d.) of 31.5±26.7% of their excess body weight (12.1±9.6% total body weight), whereas those in the Lifestyle Counseling group had lost a mean of 9.8±15.5% of their excess body weight (3.5±6.0% total body weight) (P<0.001). A total of 58.6% of participants in the AspireAssist group and 15.3% of participants in the Lifestyle Counseling group lost at least 25% of their excess body weight (P<0.001). The most frequently reported adverse events were abdominal pain and discomfort in the perioperative period and peristomal granulation tissue and peristomal irritation in the postoperative period. Serious adverse events were reported in 3.6% of participants in the AspireAssist group.
Conclusions: The AspireAssist System was associated with greater weight loss than Lifestyle Counseling alone.
Conflict of interest statement
Figures
Comment in
-
Editorial: Aspiration Therapy for Weight Loss: Is the Squeeze worth the Juice?Am J Gastroenterol. 2017 Mar;112(3):458-589. doi: 10.1038/ajg.2017.2. Am J Gastroenterol. 2017. PMID: 28270668
References
-
- Klein S, Wadden T, Sugerman HJ. American Gastroenterological Association Technical Review: clinical issues in obesity. Gastroenterology 2002;123:882–932. - PubMed
-
- Li W, Baraboi ED, Cluny NL et al. Malabsorption plays a major role in the effects of the biliopancreatic diversion with duodenal switch on energy metabolism in rats. Surg Obes Relat Dis 2015;11:356–66. - PubMed
-
- Xia Y, Kelton CM, Guo JJ et al. Treatment of obesity: pharmacotherapy trends in the United States from 1999 to 2010. Obesity 2015;23:1721–8. - PubMed
-
- Buchwald H, Oien D. Metabolic/bariatric surgery worldwide 2011. Obes Surg 2013;23:427–36. - PubMed
-
- Langeveld M, DeVries JH. The long-term effect of energy restricted diets for treating obesity. Obesity 2015;23:1529–38. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
