

Comparison of gram-negative and gram-positive hematogenous pyogenic spondylodiscitis: clinical characteristics and outcomes of treatment
- PMID: 27923346
- PMCID: PMC5139091
- DOI: 10.1186/s12879-016-2071-4
Comparison of gram-negative and gram-positive hematogenous pyogenic spondylodiscitis: clinical characteristics and outcomes of treatment
Abstract
Background: To the best of our knowledge, no study has compared gram-negative bacillary hematogenous pyogenic spondylodiscitis (GNB-HPS) with gram-positive coccal hematogenous pyogenic spondylodiscitis (GPC-HPS) regarding their clinical characteristics and outcomes.
Methods: From January 2003 to January 2013, 54 patients who underwent combined antibiotic and surgical therapy in the treatment of hematogenous pyogenic spondylodiscitis were included.
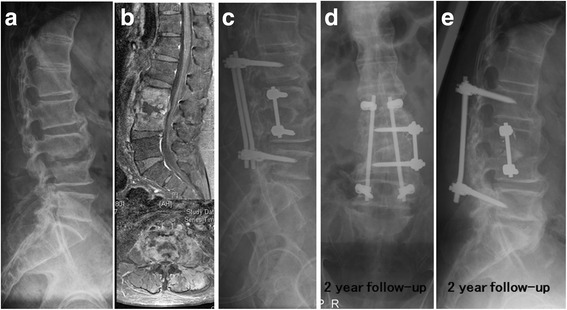
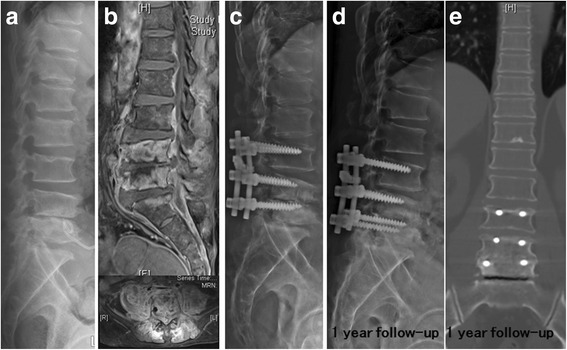
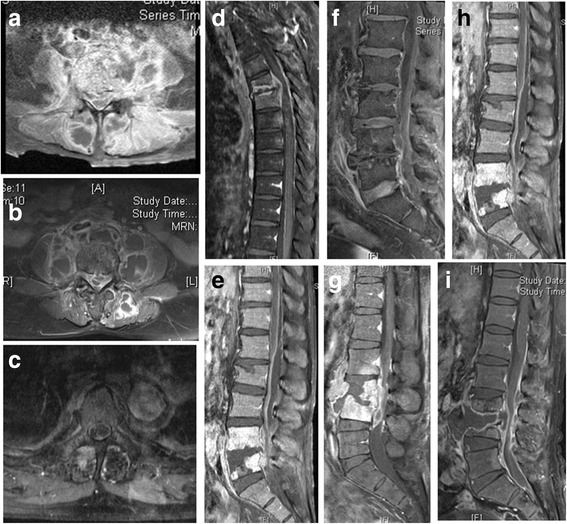
Results: Compared with 37 GPC-HPS patients, the 17 GNB-HPS patients were more often found to be older individuals, a history of cancer, and a previous history of symptomatic urinary tract infection. They also had a less incidence of epidural abscess formation compared with GPC-HPS patients from findings on magnetic resonance imaging (MRI). Constitutional symptoms were the primary reasons for initial physician visits in GNB-HPS patients whereas pain in the affected spinal region was the most common manifestation in GPC-HPS patients at initial visit. The clinical outcomes of GNB-HPS patients under combined surgical and antibiotic treatment were not different from those of GPC-HPS patients. In multivariate analysis, independent predicting risk factors for GNB-HPS included a malignant history and constitutional symptoms and that for GPC-HPS was epidural abscess.
Conclusions: The clinical manifestations and MRI presentations of GNB-HPS were distinguishable from those of GPC-HPS.
Keywords: Gram-negative infection; Gram-positive infection; Hematogenous pyogenic spondylodiscitis.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
