

To expand coverage, or increase frequency: Quantifying the tradeoffs between equity and efficiency facing cervical cancer screening programs in low-resource settings
- PMID: 27925175
- PMCID: PMC5516173
- DOI: 10.1002/ijc.30551
To expand coverage, or increase frequency: Quantifying the tradeoffs between equity and efficiency facing cervical cancer screening programs in low-resource settings
Abstract
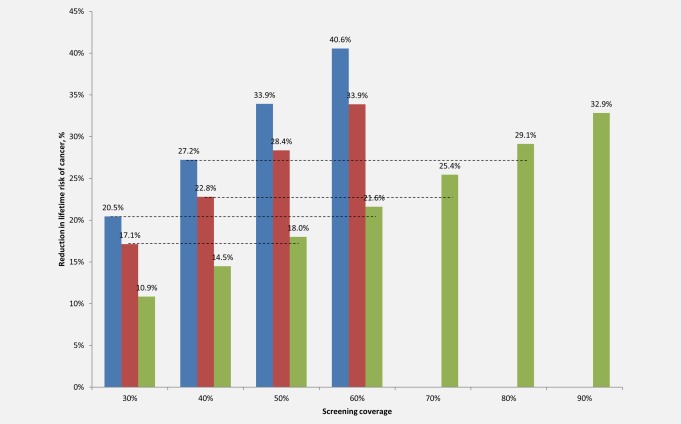
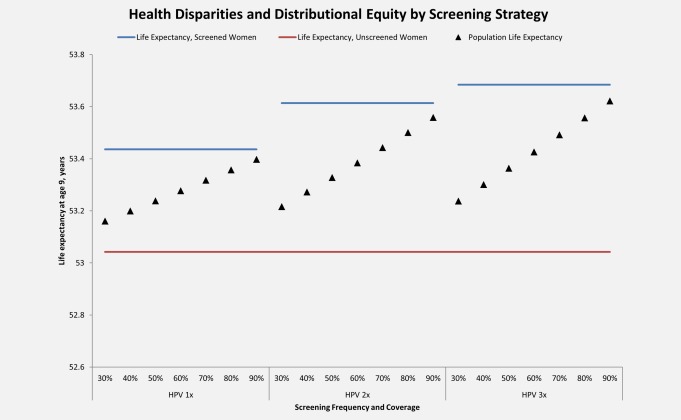
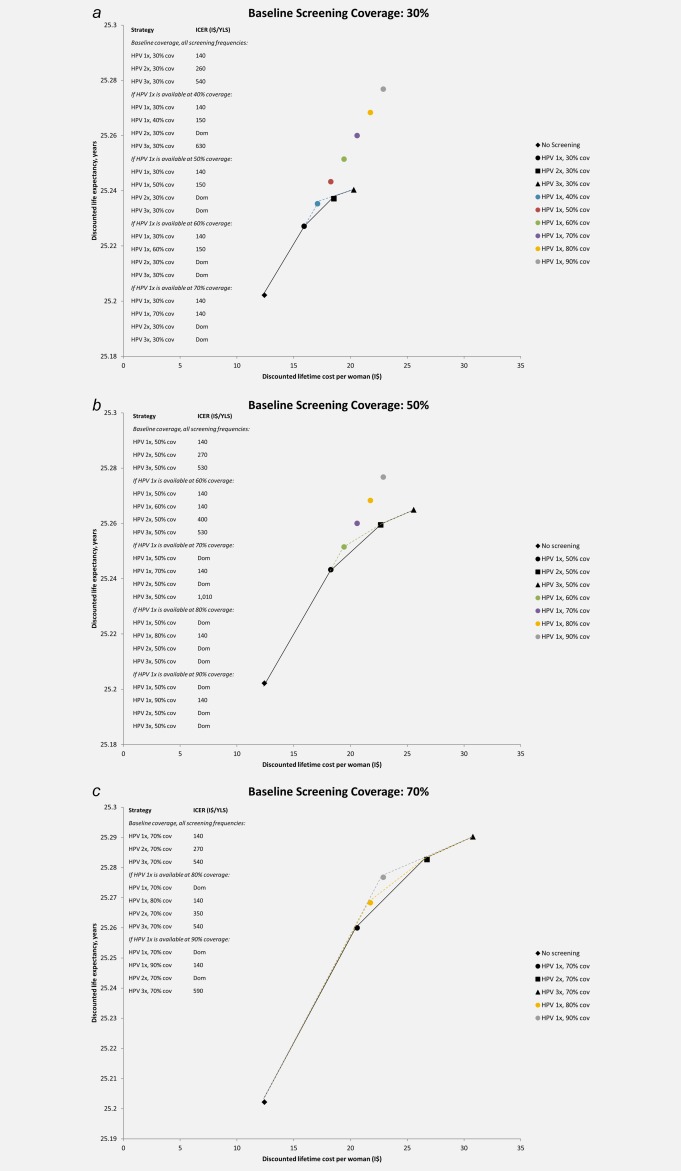
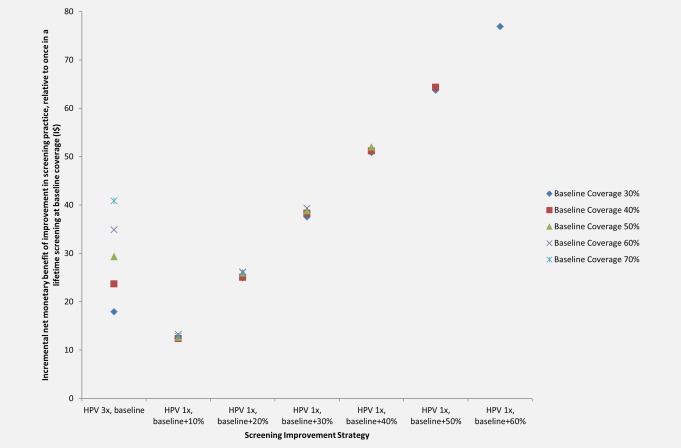
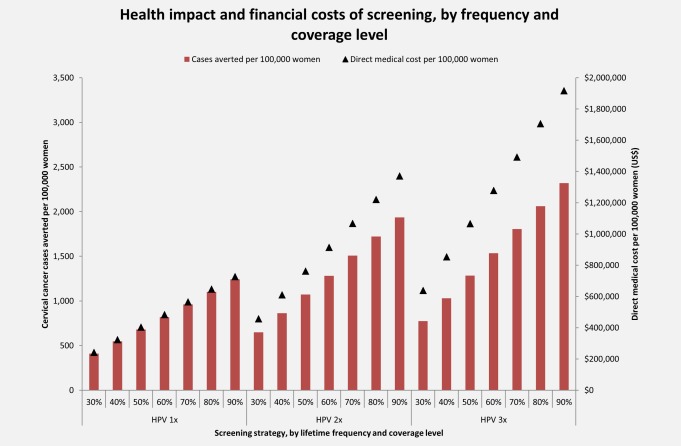
Cervical cancer is a leading cause of cancer death worldwide, with 85% of the disease burden residing in less developed regions. To inform evidence-based decision-making as cervical cancer screening programs are planned, implemented, and scaled in low- and middle-income countries, we used cost and test performance data from the START-UP demonstration project in Uganda and a microsimulation model of HPV infection and cervical carcinogenesis to quantify the health benefits, distributional equity, cost-effectiveness, and financial impact of either (1) improving access to cervical cancer screening or (2) increasing the number of lifetime screening opportunities for women who already have access. We found that when baseline screening coverage was low (i.e., 30%), expanding coverage of screening once in a lifetime to 50% can yield comparable reductions in cancer risk to screening two or three times in a lifetime at 30% coverage, lead to greater reductions in health disparities, and cost 150 international dollars (I$) per year of life saved (YLS). At higher baseline screening coverage levels (i.e., 70%), screening three times in a lifetime yielded greater health benefits than expanding screening once in a lifetime to 90% coverage, and would have a cost-effectiveness ratio (I$590 per YLS) below Uganda's per capita GDP. Given very low baseline coverage at present, we conclude that a policy focus on increasing access for previously unscreened women appears to be more compatible with improving both equity and efficiency than a focus on increasing frequency for a small subset of women.
Keywords: HPV DNA test; Uganda; cancer screening; cervical cancer; economic evaluation; health disparities; human papillomavirus.
© 2016 UICC.
Figures
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet], 2013, International Agency for Research on Cancer: Lyon, France.
-
- “FDA approves Gardasil 9 for prevention of certain cancers caused by five additional types of HPV.” FDA News Release December 11, 2014; Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm426485.htm.
-
- De Carvalho N, Teixeira J, Roteli‐Martins CM, et al. Sustained efficacy and immunogenicity of the HPV‐16/18 AS04‐adjuvanted vaccine up to 7.3 years in young adult women. Vaccine 2010;28:6247–55. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
