

Shock Wave Enhances Angiogenesis through VEGFR2 Activation and Recycling
- PMID: 27925633
- PMCID: PMC5263055
- DOI: 10.2119/molmed.2016.00108
Shock Wave Enhances Angiogenesis through VEGFR2 Activation and Recycling
Abstract
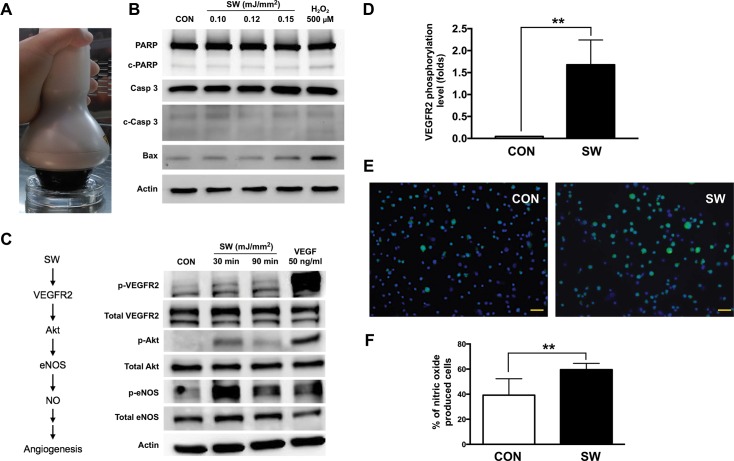
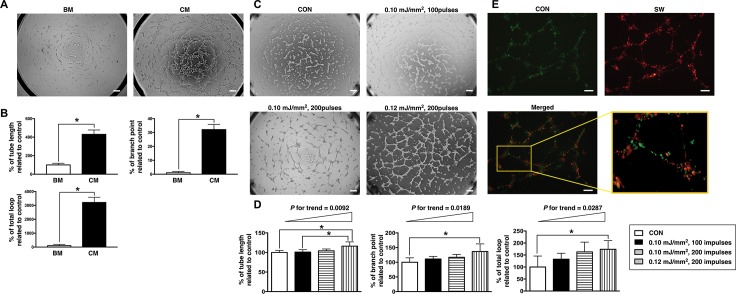
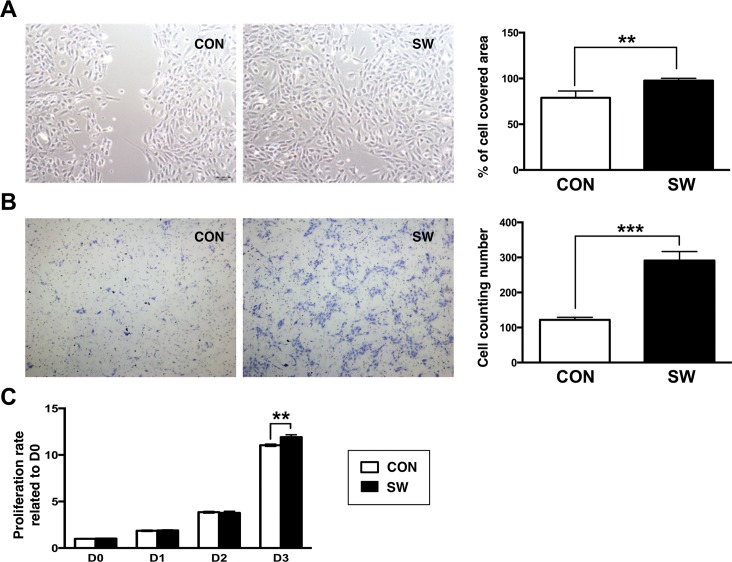
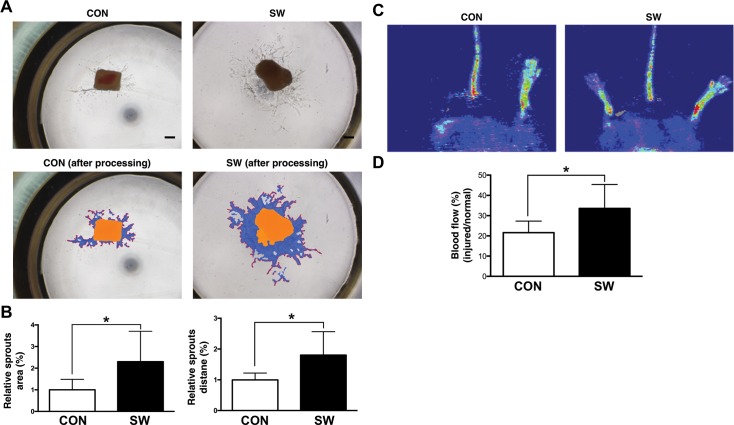
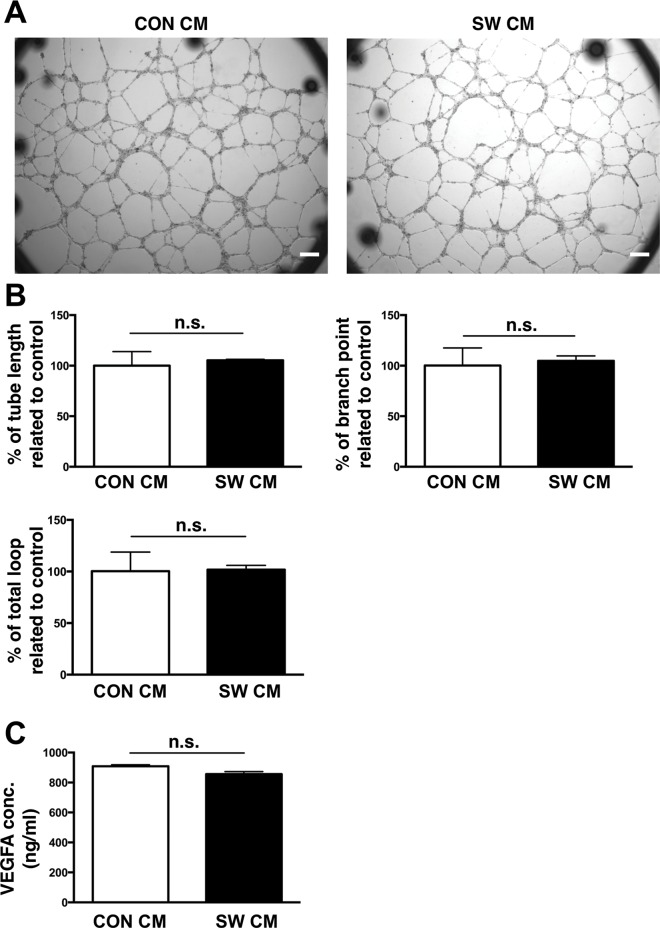
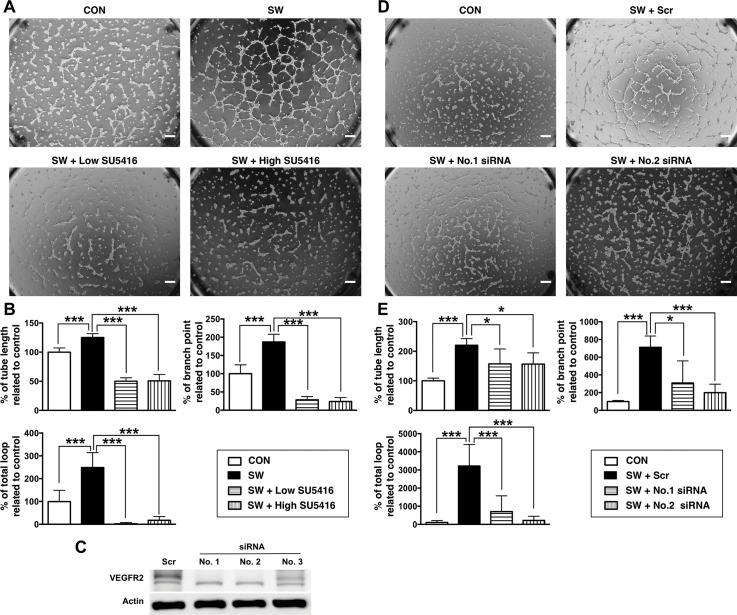
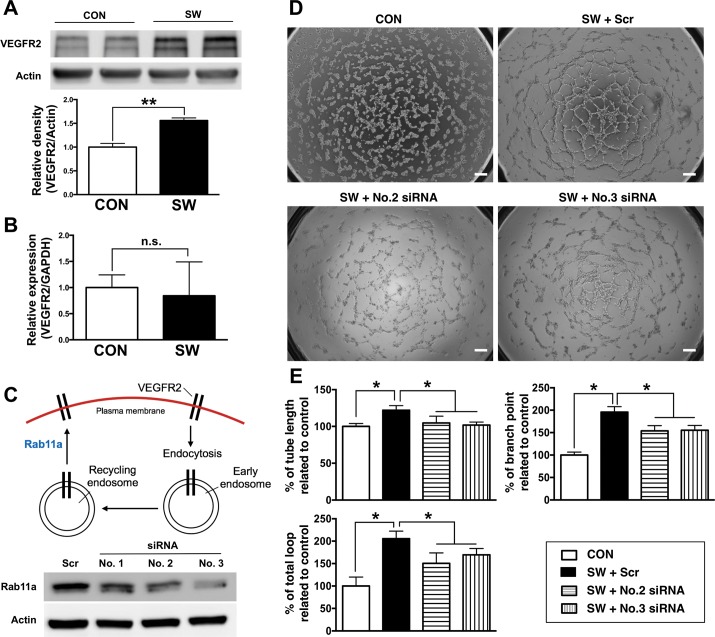
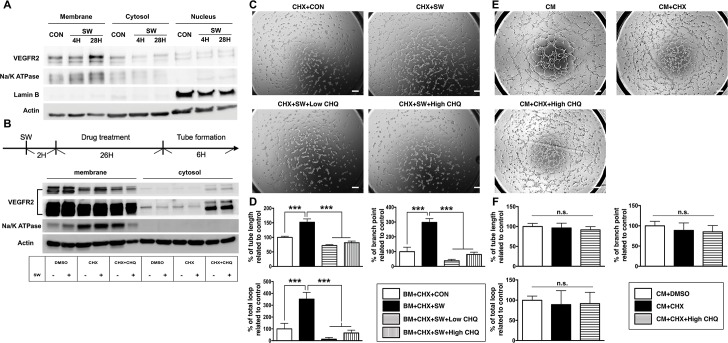
Although low-energy shock wave (SW) is adopted to treat ischemic diseases because of its pro-angiogenic properties, the underlying mechanism remains unclear. This study aimed at testing whether SW-induced angiogenesis may be through endothelial vascular endothelial growth factor receptor 2 (VEGFR2) signaling and trafficking. Phosphorylation of VEGFR2-Akt-eNOS axis and production of nitric oxide (NO) were determined in human umbilical vein endothelial cells (HUVECs) treated with SW. Carotid artery in ob/ob mice was treated with SW before evaluation with sprouting assay. Critical limb ischemia was induced in ob/ob mice to evaluate blood flow recovery after SW treatment. Tube formation and migration assays were also performed with/without SW treatment in the presence/absence of SU5416 (VEGFR2 kinase inhibitor) and siRNA-driven silencing of VEGFR2. Chloroquine was used for disrupting endosome, and Rab11a controlling slow endocytic recycling was silenced with siRNA in vitro. Following SW treatment, augmented ligand-independent phosphorylation in VEGFR2-Akt-eNOS axis and endogenous NO production, increased cellular migration and tube formation, elevated sprouting of carotid artery and blood flow in ischemic limb in ob/ob mice were noted. Moreover, SU5416 and VEGFR2 silencing both inhibited SW-induced angiogenesis. SW-induced angiogenesis, which was accompanied by increased VEGFR2 protein expression without transcriptional change, was suppressed by chloroquine and Rab11a silencing. We concluded that SW enhanced angiogenesis via ligand-independent activation of VEGFR2 and further prolonged through endosome-to-plasma membrane recycling in endothelial cells.
Keywords: VEGFR2; angiogenesis; endocytic recycling; endothelial cell; shock wave.
Conflict of interest statement
The authors declare they have no competing interests as defined by
Figures
References
-
- Langer PR. Two emerging technologies for Achilles tendinopathy and plantar fasciopathy. Clin Podiatr Med Surg. 2015;32:183–93. - PubMed
-
- Mani-Babu S, Morrissey D, Waugh C, Screen H, Barton C. The effectiveness of extracorporeal shock wave therapy in lower limb tendinopathy: a systematic review. Am J Sports Med. 2015;43:752–61. - PubMed
-
- Wang CJ, Wang FS, Yang KD, Weng LH, Ko JY. Long-term results of extracorporeal shockwave treatment for plantar fasciitis. Am J Sports Med. 2006;34:592–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
