

Viral oncoprotein antibodies as a marker for recurrence of Merkel cell carcinoma: A prospective validation study
- PMID: 27925665
- PMCID: PMC5384867
- DOI: 10.1002/cncr.30475
Viral oncoprotein antibodies as a marker for recurrence of Merkel cell carcinoma: A prospective validation study
Abstract
Background: Merkel cell carcinoma (MCC) is an aggressive skin cancer with a recurrence rate of >40%. Of the 2000 MCC cases per year in the United States, most are caused by the Merkel cell polyomavirus (MCPyV). Antibodies to MCPyV oncoprotein (T-antigens) have been correlated with MCC tumor burden. The present study assesses the clinical utility of MCPyV-oncoprotein antibody titers for MCC prognostication and surveillance.
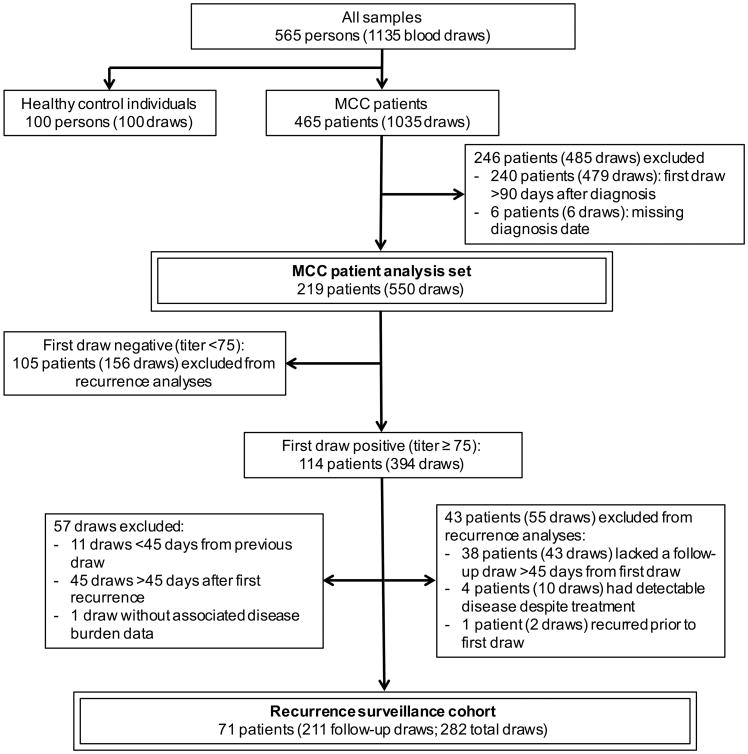
Methods: MCPyV-oncoprotein antibody detection was optimized in a clinical laboratory. A cohort of 219 patients with newly diagnosed MCC were followed prospectively (median follow-up, 1.9 years). Among the seropositive patients, antibody titer and disease status were serially tracked.
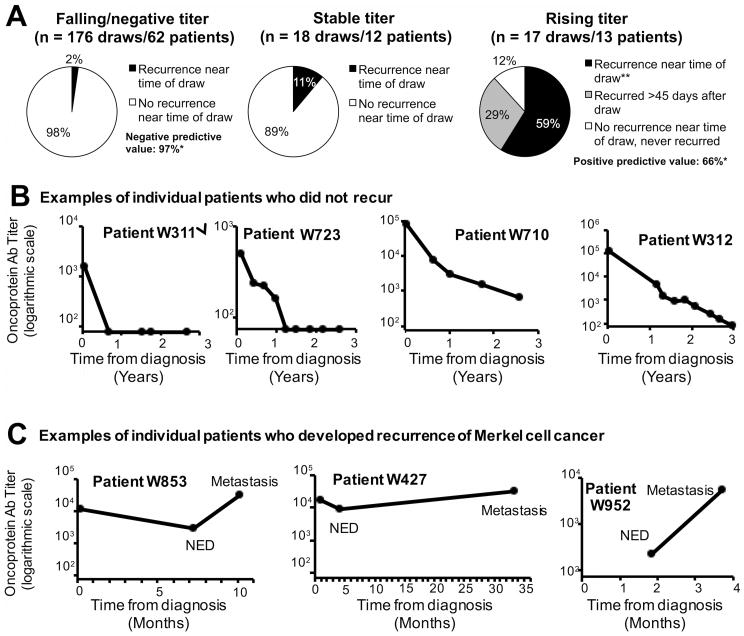
Results: Antibodies to MCPyV oncoproteins were rare among healthy individuals (1%) but were present in most patients with MCC (114 of 219 patients [52%]; P < .01). Seropositivity at diagnosis independently predicted decreased recurrence risk (hazard ratio, 0.58; P = .04) in multivariate analyses adjusted for age, sex, stage, and immunosuppression. After initial treatment, seropositive patients whose disease did not recur had rapidly falling titers that became negative by a median of 8.4 months. Among seropositive patients who underwent serial evaluation (71 patients; 282 time points), an increasing oncoprotein titer had a positive predictive value of 66% for clinically evident recurrence, whereas a decreasing titer had a negative predictive value of 97%.
Conclusions: Determination of oncoprotein antibody titer assists in the clinical management of patients with newly diagnosed MCC by stratifying them into a higher risk seronegative cohort, in which radiologic imaging may play a more prominent role, and into a lower risk seropositive cohort, in which disease status can be tracked in part by oncoprotein antibody titer. Cancer 2017;123:1464-1474. © 2016 American Cancer Society.
Keywords: Merkel cell carcinoma (MCC); Merkel cell polyomavirus (MCPyV); T antigen; oncoprotein; serology; skin cancer.
© 2016 American Cancer Society.
Conflict of interest statement
Conflicts of interest: None
Figures

References
-
- Albores-Saavedra J, Batich K, Chable-Montero F, Sagy N, Schwartz AM, Henson DE. Merkel cell carcinoma demographics, morphology, and survival based on 3870 cases: a population based study. J Cutan Pathol. 2010;37:20–27. - PubMed
-
- United States Census Population Clock. [accessed August 17, 2015]; Available from URL: http://www.census.gov/popclock/
-
- Brewer JD, Shanafelt TD, Otley CC, et al. Chronic lymphocytic leukemia is associated with decreased survival of patients with malignant melanoma and Merkel cell carcinoma in a SEER population-based study. J Clin Oncol. 2012;30:843–849. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
