

Minimally invasive oesophagectomy versus open esophagectomy for resectable esophageal cancer: a meta-analysis
- PMID: 27927246
- PMCID: PMC5143462
- DOI: 10.1186/s12957-016-1062-7
Minimally invasive oesophagectomy versus open esophagectomy for resectable esophageal cancer: a meta-analysis
Abstract
Background: Open esophagectomy (OE) is associated with significant morbidity and mortality. Minimally invasive oesophagectomy (MIO) reduces complications in resectable esophageal cancer. The aim of this study is to explore the superiority of MIO in reducing complications and in-hospital mortality than OE.
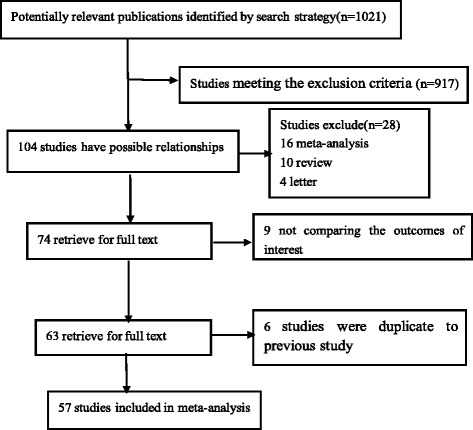
Methods: MEDLINE, Embase, Science Citation Index, Wanfang, and Wiley Online Library were thoroughly searched. Odds ratio (OR)/weighted mean difference (WMD) with a 95% confidence interval (CI) was used to assess the strength of association.
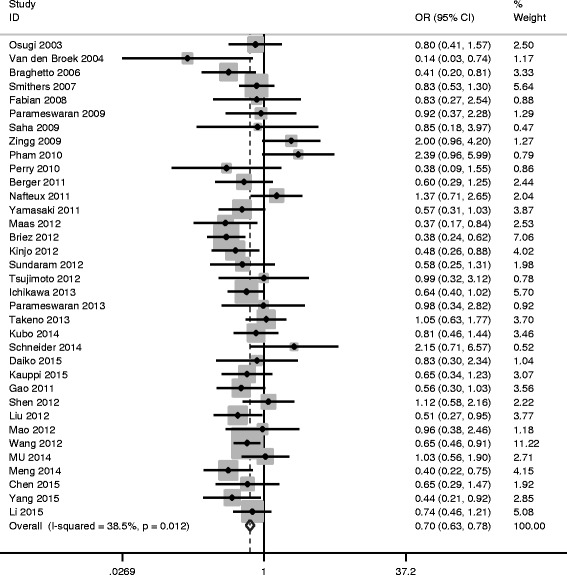
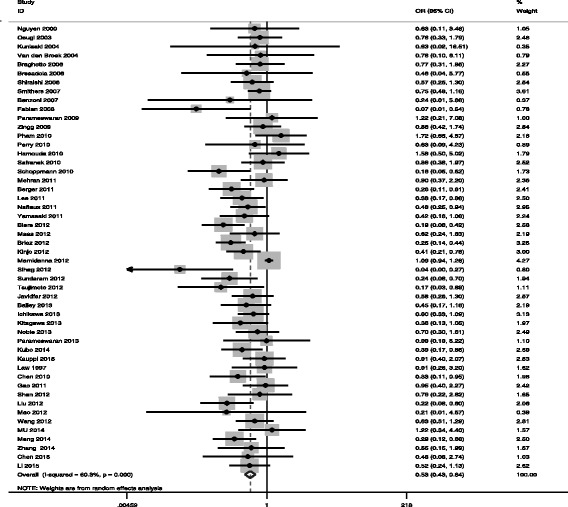
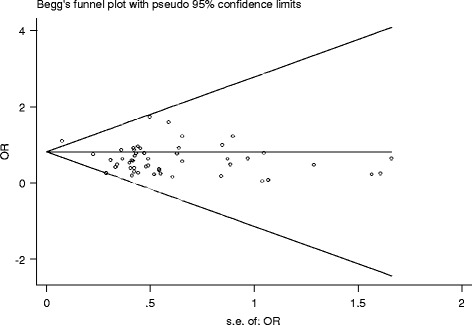
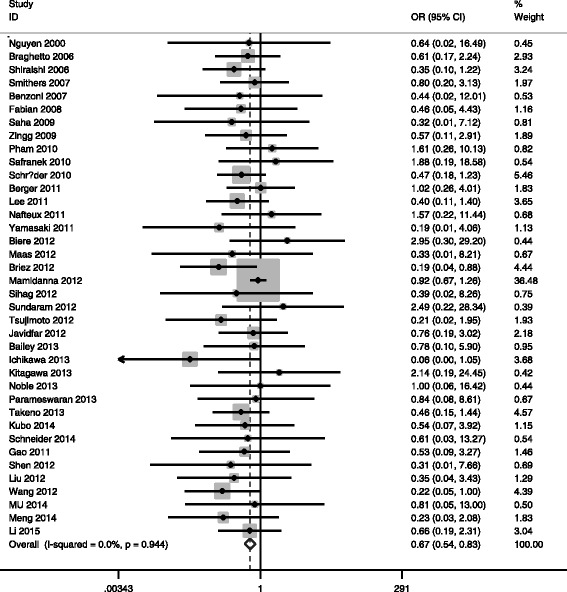
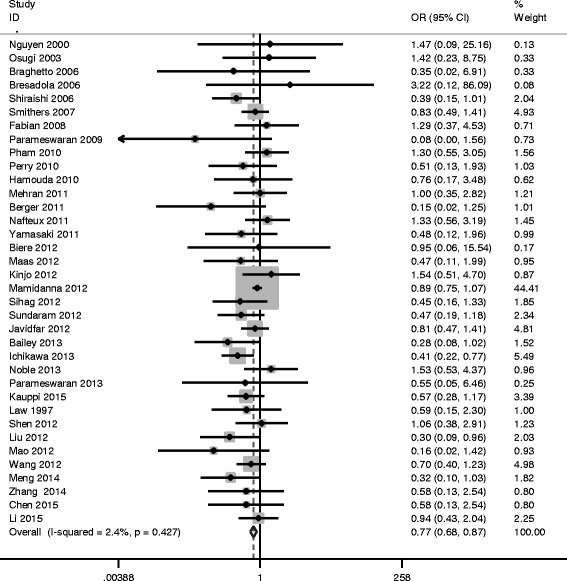
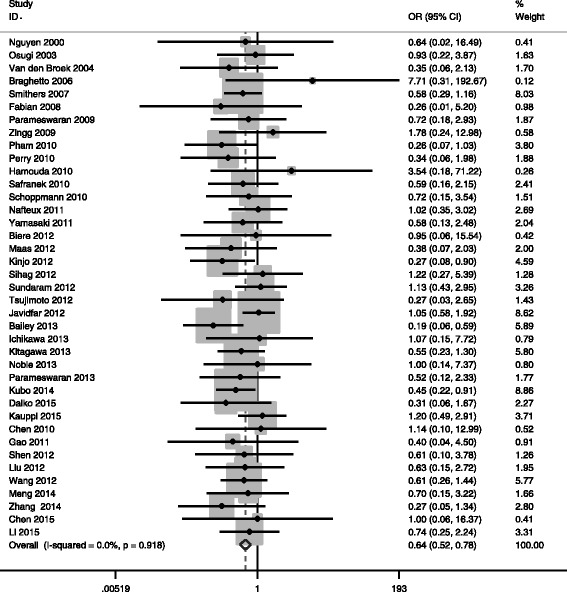
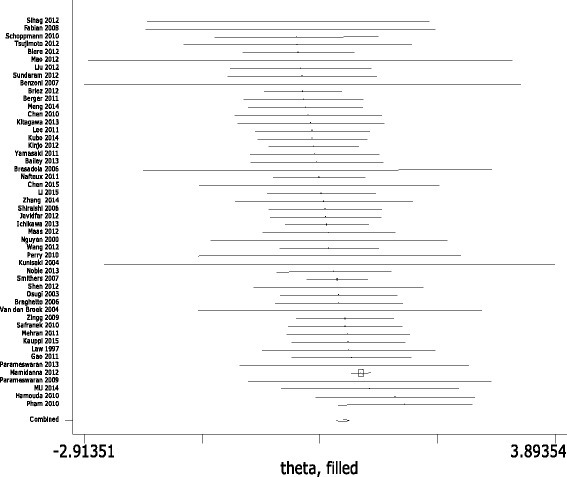
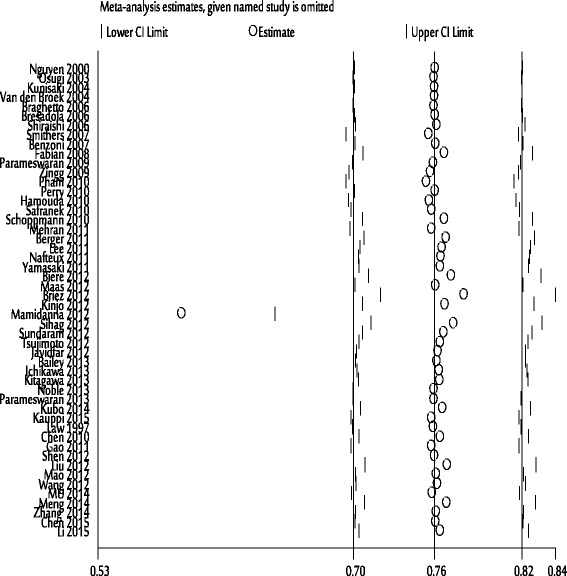
Results: Fifty-seven studies containing 15,790 cases of resectable esophageal cancer were included. MIO had less intraoperative blood loss, short hospital stay, and high operative time (P < 0.05) than OE. MIO also had reduced incidence of total complications; (OR = 0.700, 95% CI = 0.626 ~ 0.781, P V < 0.05), pulmonary complications (OR = 0.527, 95% CI = 0431 ~ 0.645, P V < 0.05), cardiovascular complications (OR = 0.770, 95% CI = 0.681 ~ 0.872, P V < 0.05), and surgical technology related (STR) complications (OR = 0.639, 95% CI = 0.522 ~ 0.781, P V < 0.05), as well as lower in-hospital mortality (OR = 0.668, 95% CI = 0.539 ~ 0.827, P V < 0.05). However, the number of harvested lymph nodes, intensive care unit (ICU) stay, gastrointestinal complications, anastomotic leak (AL), and recurrent laryngeal nerve palsy (RLNP) had no significant difference.
Conclusions: MIO is superior to OE in terms of perioperative complications and in-hospital mortality.
Keywords: Complications; Minimally invasive esophagectomy; Mortality; Open esophagectomy.
Figures
References
-
- Morita M, Nakanoko T, Fujinaka Y, Kubo N, Yamashita N, Yoshinaga K, Saeki H, Emi Y, Kakeji Y, Shirabe K, Maehara Y. In-hospital mortality after a surgical resection for esophageal cancer: analyses of the associated factors and historical changes. Ann Surg Oncol. 2011;18:1757–1765. doi: 10.1245/s10434-010-1502-5. - DOI - PubMed
-
- Hulscher JB, van Sandick JW, de Boer AG, Wijnhoven BP, Tijssen JG, Fockens P, Stalmeier PF, Ten KF, van Dekken H, Obertop H, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002;347:1662–1669. doi: 10.1056/NEJMoa022343. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
