

Albuminuria changes are associated with subsequent risk of end-stage renal disease and mortality
- PMID: 27927597
- PMCID: PMC5523054
- DOI: 10.1016/j.kint.2016.09.037
Albuminuria changes are associated with subsequent risk of end-stage renal disease and mortality
Abstract
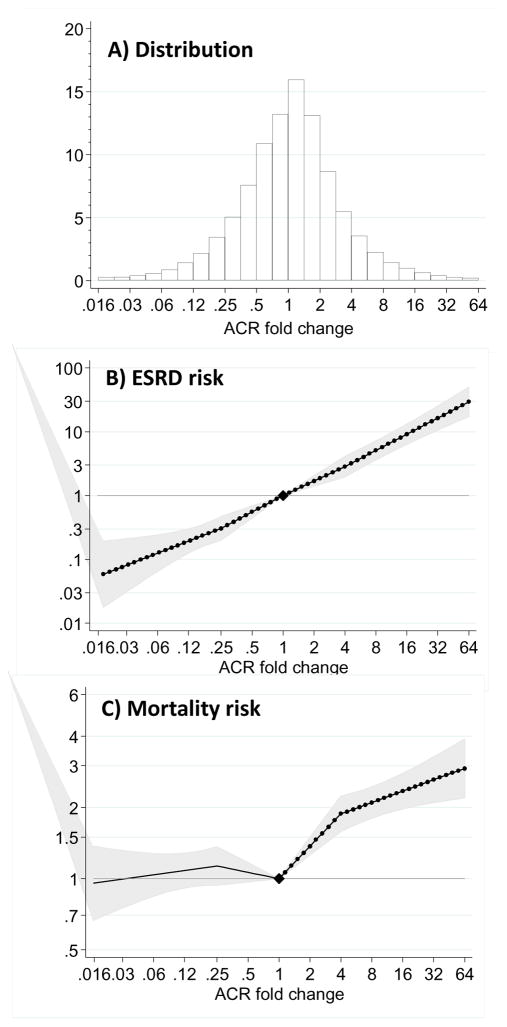
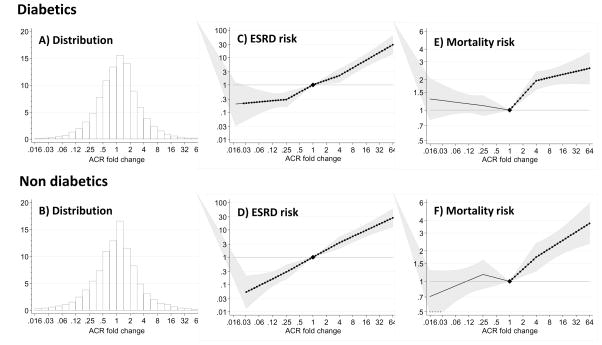
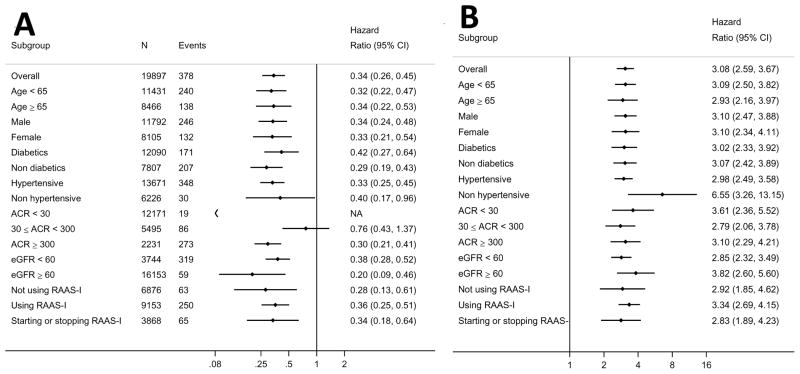
Current guidelines for chronic kidney disease (CKD) recommend using albuminuria as well as estimated glomerular filtration rate (eGFR) to stage CKD. However, CKD progression is solely defined by change in eGFR with little regard to the risk implications of change in albuminuria. This is an observational study from the Stockholm CREAtinine Measurements (SCREAM) project, a health care utilization cohort from Stockholm, Sweden, with laboratory measures from 2006-2011 and follow-up through December 2012. Included were 31,732 individuals with two or more ambulatory urine albumin to creatinine ratio (ACR) tests. We assessed the association between change in ACR during a baseline period of 1, 2, or 3 years and end-stage renal disease (ESRD) or death. Using a 2-year baseline period, there were 378 ESRD events and 1712 deaths during a median of 3 years of follow-up. Compared to stable ACR, a 4-fold increase in ACR was associated with a 3.08-times (95% confidence interval 2.59 to 3.67) higher risk of ESRD while a 4-fold decrease in ACR was associated with a 0.34-times (0.26 to 0.45) lower risk of ESRD. Similar associations were found in people with and without diabetes mellitus, with and without hypertension, and also when adjusted for the change in eGFR during the same period. The association between change in ACR and mortality was weaker: ACR increase was associated with mortality, but the relationship was largely flat for ACR decline. Results were consistent for 1-, 2-, and 3-year ACR changes. Thus, changes in albuminuria are strongly and consistently associated with the risk of ESRD and death.
Keywords: albuminuria; changes in albuminuria; death; end-stage renal disease; estimated glomerular filtration rate.
Copyright © 2016 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Eckardt KU, Coresh J, Devuyst O, et al. Evolving importance of kidney disease: from subspecialty to global health burden. Lancet. 2013;382:158–169. - PubMed
-
- K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39:S1–266. - PubMed
-
- Stevens PE, Levin A. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Annals of internal medicine. 2013;158:825–830. - PubMed
-
- KDIGO clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:1–150. - PubMed
-
- Qaseem A, Hopkins RH, Jr, Sweet DE, et al. Screening, monitoring, and treatment of stage 1 to 3 chronic kidney disease: A clinical practice guideline from the American College of Physicians. Annals of internal medicine. 2013;159:835–847. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
