

What Is the More Effective Antibiotic Stewardship Intervention: Preprescription Authorization or Postprescription Review With Feedback?
- PMID: 27927861
- PMCID: PMC6248350
- DOI: 10.1093/cid/ciw780
What Is the More Effective Antibiotic Stewardship Intervention: Preprescription Authorization or Postprescription Review With Feedback?
Erratum in
-
Erratum.Clin Infect Dis. 2017 Nov 13;65(11):1961. doi: 10.1093/cid/cix758. Clin Infect Dis. 2017. PMID: 29140518 Free PMC article. No abstract available.
Abstract
Background: The optimal approach to conducting antibiotic stewardship interventions has not been defined. We compared days of antibiotic therapy (DOT) using preprescription authorization (PPA) vs postprescription review with feedback (PPRF) strategies.
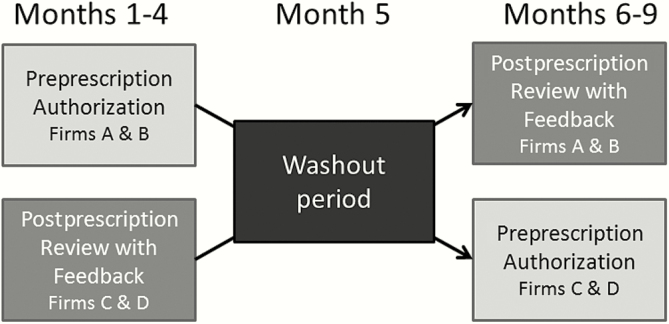
Methods: A quasi-experimental, crossover trial comparing PPA and PPRF for adult inpatients prescribed any antibiotic was conducted. For the first 4 months, 2 medicine teams were assigned to the PPA arm and the other 2 teams to the PPRF arm. The teams were then assigned to the alternate arm for an additional 4 months. Appropriateness of antibiotic use was adjudicated by at least 2 infectious diseases-trained clinicians and according to institutional guidelines.
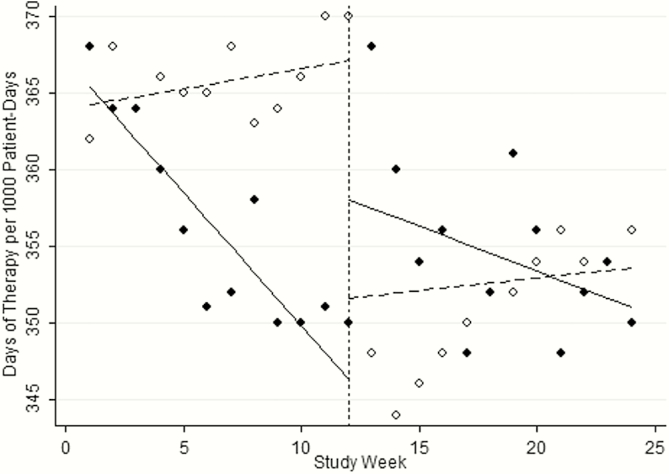
Results: There were 2686 and 2693 patients admitted to the PPA and PPRF groups, with 29% and 27% of patients prescribed antibiotics, respectively. Initially, antibiotic DOTs remained relatively unchanged in the PPA arm. When changed to the PPRF arm, antibiotic use decreased (-2.45 DOT per 1000 patient-days [PD]). In the initial PPRF arm, antibiotic use decreased (slope of -5.73 DOT per 1000 PD) but remained constant when changed to the PPA arm. Median patient DOTs in the PPA and PPRF arms were 8 and 6 DOT per 1000 PD, respectively (P = .03). Antibiotic therapy was guideline-noncompliant in 34% and 41% of patients on days 1 and 3 in the PPA group (P < .01) and in 57% and 36% of patients on days 1 and 3 in the PPRF group (P = .03).
Conclusions: PPRF may have more of an impact on decreasing antibiotic DOTs compared with PPA. This information may be useful for institutions without sufficient resources to incorporate both stewardship approaches.
Keywords: ASP; antibiotics; antimicrobial stewardship.; days of therapy.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Time Efficiency Assessment of Antimicrobial Stewardship Strategies.Clin Infect Dis. 2017 May 15;64(10):1463-1464. doi: 10.1093/cid/cix220. Clin Infect Dis. 2017. PMID: 28329195 Free PMC article. No abstract available.
References
-
- Malani AN, Richards PG, Kapila S, Otto MH, Czerwinski J, Singal B. Clinical and economic outcomes from a community hospital’s antimicrobial stewardship program. Am J Infect Control 2013; 41:145–8. - PubMed
-
- Solomon DH, Van Houten L, Glynn RJ, et al. Academic detailing to improve use of broad-spectrum antibiotics at an academic medical center. Arch Intern Med 2001; 161:1897–902. - PubMed
-
- Carling P, Fung T, Killion A, Terrin N, Barza M. Favorable impact of a multidisciplinary antibiotic management program conducted during 7 years. Infect Control Hosp Epidemiol 2003; 24:699–706. - PubMed
-
- Elligsen M, Walker SA, Pinto R, et al. Audit and feedback to reduce broad-spectrum antibiotic use among intensive care unit patients: a controlled interrupted time series analysis. Infect Control Hosp Epidemiol 2012; 33:354–61. - PubMed
-
- Laible BR, Nazir J, Assimacopoulos AP, Schut J. Implementation of a pharmacist-led antimicrobial management team in a community teaching hospital: use of pharmacy residents and pharmacy students in a prospective audit and feedback approach. J Pharm Pract 2010; 23:531–5. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
