

Review
doi: 10.3109/01658107.2014.963252.
eCollection 2015 Feb.
Microvascular Non-Arteritic Ocular Motor Nerve Palsies-What We Know and How Should We Treat?
Affiliations
- PMID: 27928323
- PMCID: PMC5123092
- DOI: 10.3109/01658107.2014.963252
Item in Clipboard
Review
Microvascular Non-Arteritic Ocular Motor Nerve Palsies-What We Know and How Should We Treat?
Neuroophthalmology.
.
Abstract
Patients with isolated unilateral pupil-sparing third or isolated fourth or sixth nerve palsies over 50 years are often diagnosed with "microvascular extraocular palsies". This condition and its management provoke divergent opinions. We review the literature and describe the incidence, pathology, clinical presentation, yield of imaging, and management. A retrospective diagnosis of exclusion has little practical use. We suggest a pragmatic approach to diagnosis, investigation, and management from initial presentation.
Keywords: Abducens; cranial nerve; microvascular ischaemia; oculomotor; trochlear.
Figures
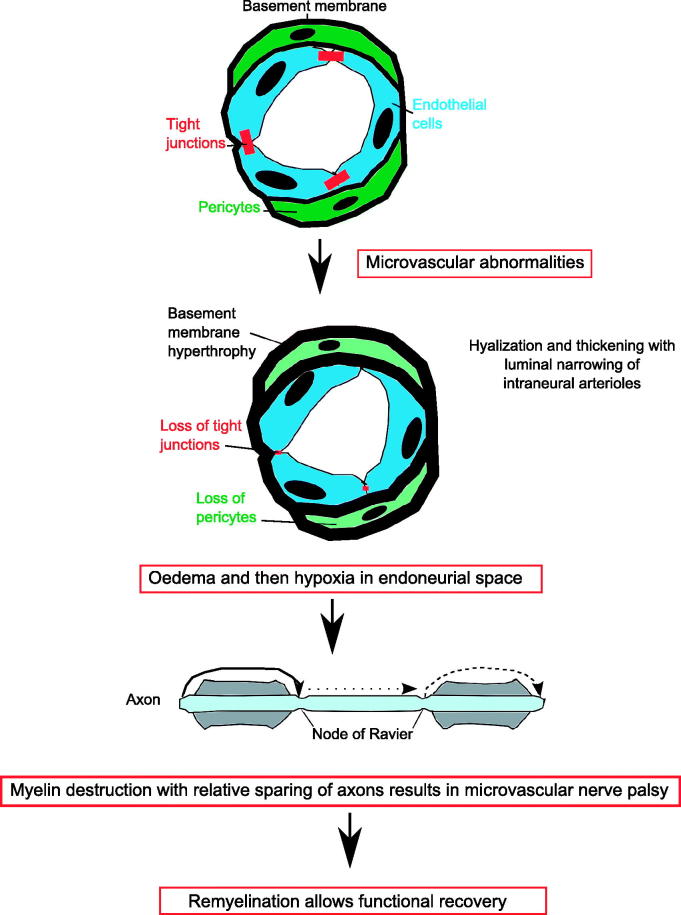
Pathophysiology of microvascular ischaemia. The blood supply to cranial nerves is via an intraneural plexus. There is a blood-nerve barrier. Microvascular abnormalities in diabetics occur due the alterations in the blood-nerve barrier resulting in loss of tight junctions, hypertrophy of the microvascular basement membrane, and loss of microvascular pericytes.8 This may underlie the hyalinzation seen in the post-mortem studies and results in oedema and then hypoxia in the endoneurial space, which causes demyelination and conduction block.5 This prevents salutatory conduction down the axon and paralysis of the extraocular muscles and microvascular nerve palsy. As remyelination occurs, there is complete functional recovery.
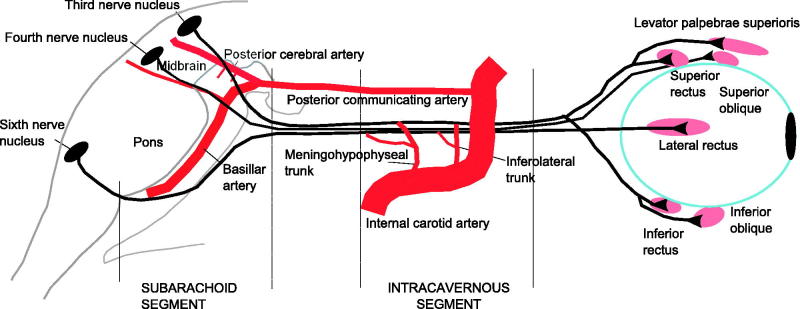
Extraneural blood supply to third, fourth, and sixth nerves. In the third nerve, the proximal segment is primarily supplied by thalamoperformating arteries (from the posterior cerebral artery) and supplemented by brainstem vessels. The middle section does not have an extraneural supply but depends on intraneural plexus and the distal (or intracavernous) section is primarily supplied by the inferior cavernous sinus artery (also called inferolateral trunk) and supplemented from the menigohypophyseal trunk (branches of the internal carotid artery). In the fourth nerve, the proximal nerve received branches from the inferolateral trunk in 80% and from the tentorial artery of the meningohypophyseal trunk in 20%. The distal half was supplied by the branches from the inferolateral trunk only. In the sixth nerve, the proximal third received branches from the dorsal clival artery of the meningohypophyseal trunk. The middle and distal thirds received branches from the inferior cavernous sinus artery (also called inferolateral trunk).
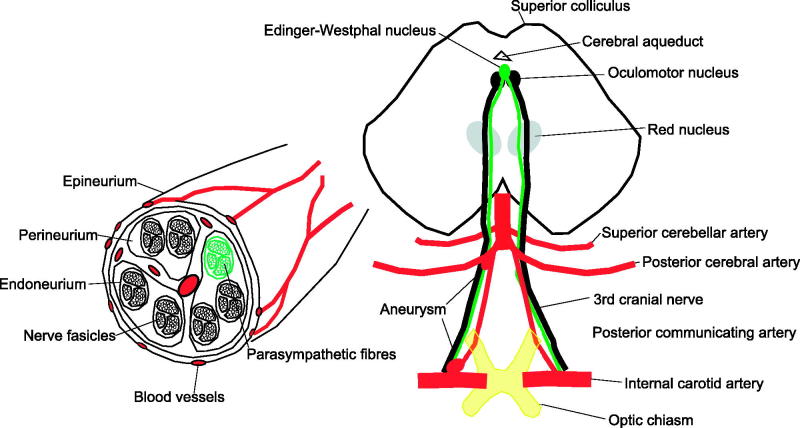
Significance of pupil involvement. Third nerve palsies often have pupillary involvement because the parasympathetic nerves innervating the iris travel with the third nerve. Pupillary involvement is an important diagnostic sign, as usually compressive lesions involve the pupil, whereas microvascular palsies do not. The parasympathetic fibres that control pupillary constriction originate in the Edinger–Westphal nucleus in the midbrain (green/light grey). These fibres then run in the superficial medial portion of the third nerve as it travels in the subarachnoid space and therefore are susceptible to compression from aneurysms arising from the nearby posterior communicating artery aneurysm. A complete third nerve palsy that spares the pupil is not caused by compression from an aneurysm because the parasympathetics fibres are located near the surface of the nerve, and if the nerve compression is severe enough to cause complete paralysis of the extraocular muscles, then the parasympathetic fibres must also be compressed. However, the microvascular pathology affects the blood vessels inside the nerve and therefore could affect all fibres travelling to the muscles and spare the superficial parasymapthetics. If the third nerve palsy is partial and spares the pupil, it is possible it is missing the parasympathetic fibres so could be caused by an aneurysm.
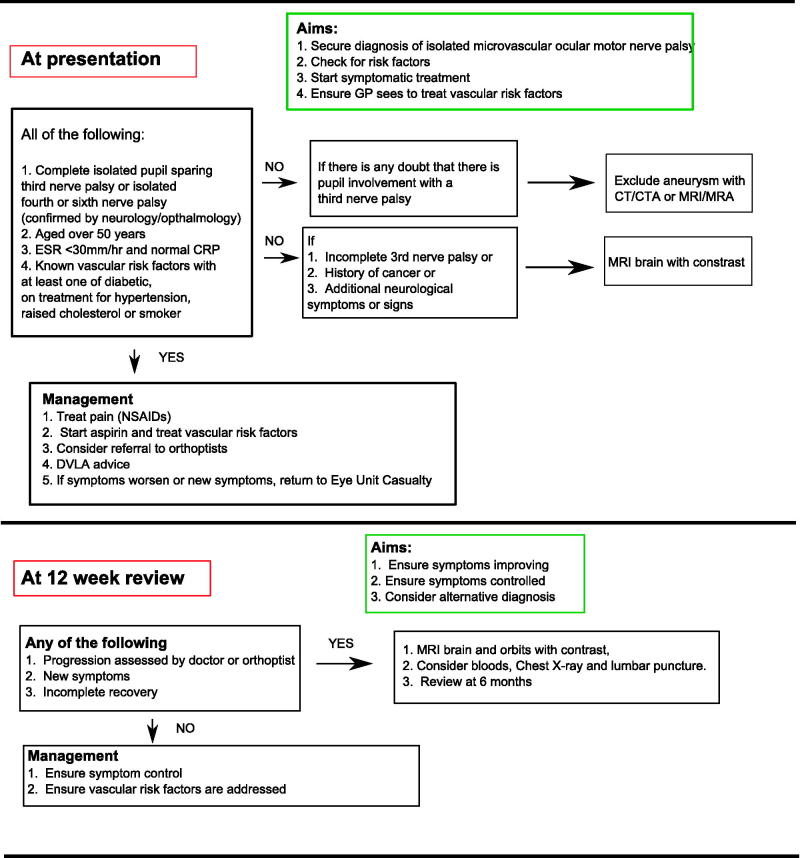
Management of microvascular nerve palsies.
References
-
- Patel SV, Mutyala S, Leske DA, Hodge DO, Holmes JM. Incidence, associations, and evaluation of sixth nerve palsy using a population-based method. Ophthalmology 2004;111:369–375 - PubMed
-
- Akagi T, Miyamoto K, Kashii S, Yoshimura N. Cause and prognosis of neurologically isolated third, fourth, or sixth cranial nerve dysfunction in cases of oculomotor palsy. Jpn J Ophthalmol 2008;52:32–35 - PubMed
-
- Park UC, Kim SJ, Hwang JM, Yu YS. Clinical features and natural history of acquired third, fourth, and sixth cranial nerve palsy. Eye (Lond) 2008;22:691–696 - PubMed
-
- Chou KL, Galetta SL, Liu GT, Volpe NJ, Bennett JL, Asbury AK, Balcer LJ. Acute ocular motor mononeuropathies: prospective study of the roles of neuroimaging and clinical assessment. J Neurol Sci 2004;219:35–39 - PubMed
-
- Asbury AK, Algredge H, Hershberg R, Miller Fischer C. Oculomotor palsy in diabetes mellitus: a clinico-pathological study. Brain 1970;93:555–566 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources