

Major Depression as a Complex Dynamic System
- PMID: 27930698
- PMCID: PMC5145163
- DOI: 10.1371/journal.pone.0167490
Major Depression as a Complex Dynamic System
Abstract
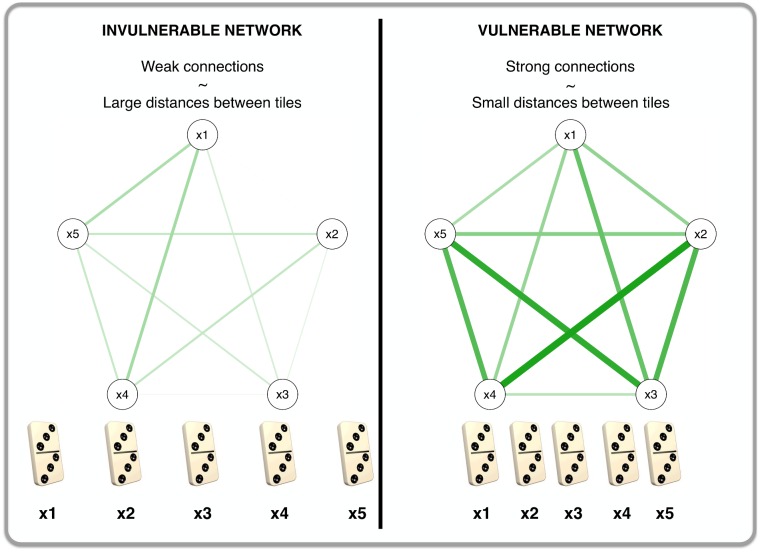
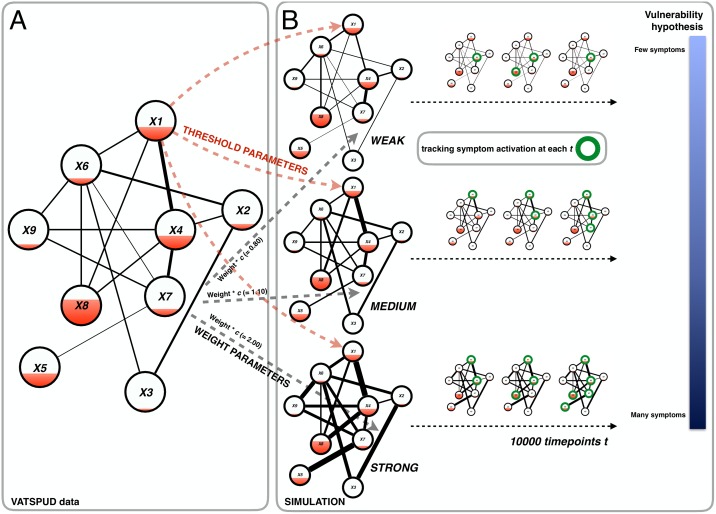
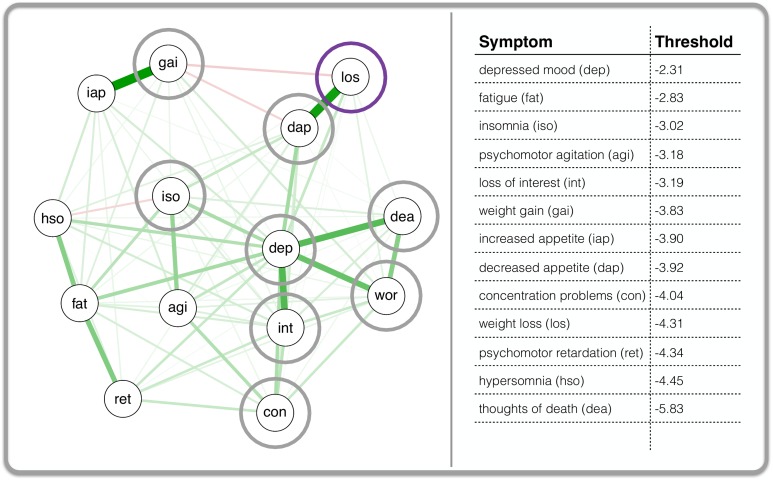
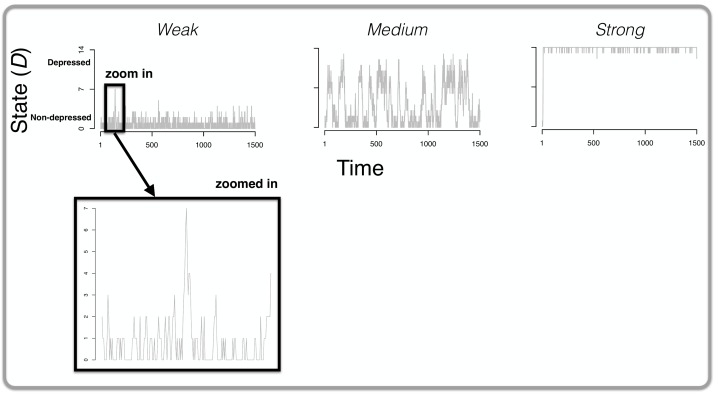
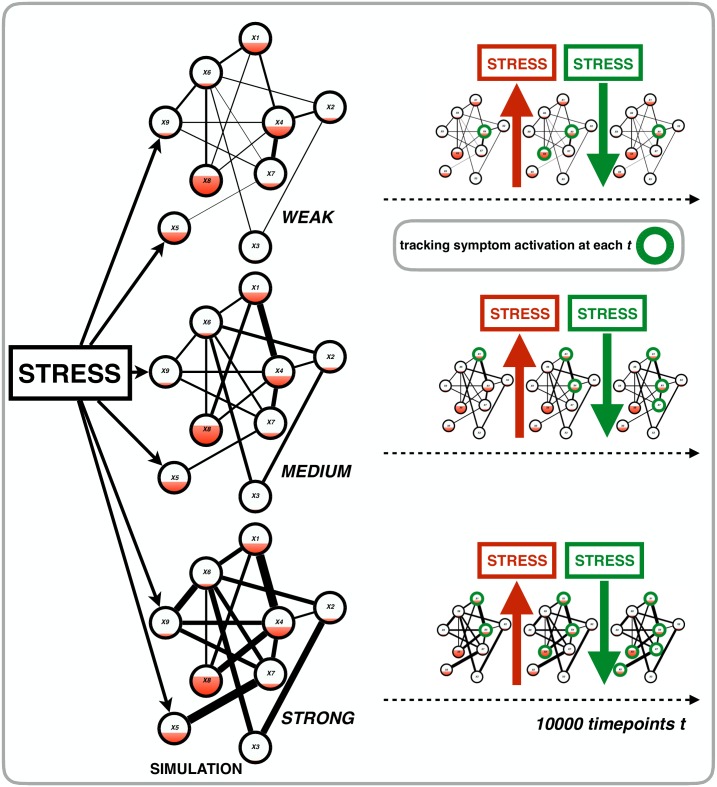
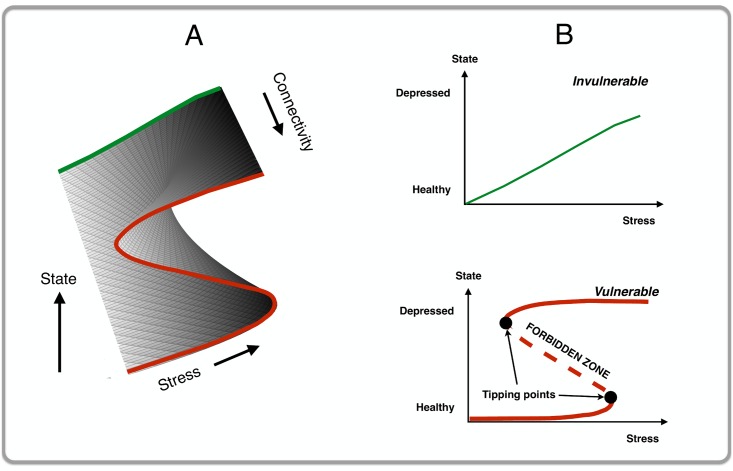
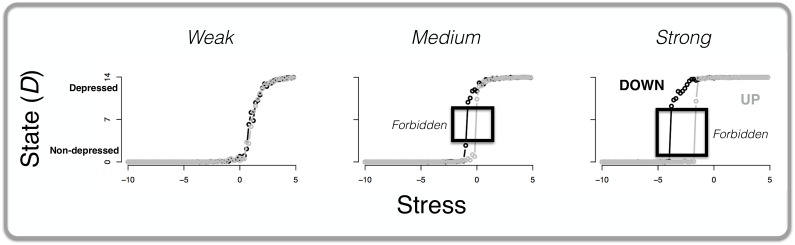
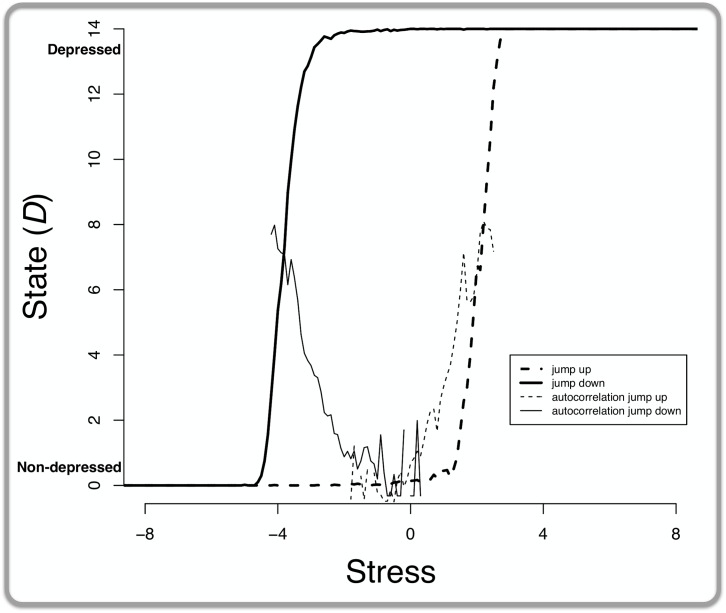
In this paper, we characterize major depression (MD) as a complex dynamic system in which symptoms (e.g., insomnia and fatigue) are directly connected to one another in a network structure. We hypothesize that individuals can be characterized by their own network with unique architecture and resulting dynamics. With respect to architecture, we show that individuals vulnerable to developing MD are those with strong connections between symptoms: e.g., only one night of poor sleep suffices to make a particular person feel tired. Such vulnerable networks, when pushed by forces external to the system such as stress, are more likely to end up in a depressed state; whereas networks with weaker connections tend to remain in or return to a non-depressed state. We show this with a simulation in which we model the probability of a symptom becoming 'active' as a logistic function of the activity of its neighboring symptoms. Additionally, we show that this model potentially explains some well-known empirical phenomena such as spontaneous recovery as well as accommodates existing theories about the various subtypes of MD. To our knowledge, we offer the first intra-individual, symptom-based, process model with the potential to explain the pathogenesis and maintenance of major depression.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Greden JF. The burden of recurrent depression: Causes, consequences, and future prospects. J Clin Psychiatry. 2001;62: 5–9. - PubMed
-
- Hammen CL, Peters SD. Interpersonal consequences of depression: Responses to men and women enacting a depressed role. J Abnorm Psychol. 1978;87: 322–332. - PubMed
-
- Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. The Lancet. 2013;382(9904): 1575–1586. - PubMed
-
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51: 8–19. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
