

Radiobiology in Cardiovascular Imaging
- PMID: 27931527
- PMCID: PMC5877470
- DOI: 10.1016/j.jcmg.2016.09.012
Radiobiology in Cardiovascular Imaging
Abstract
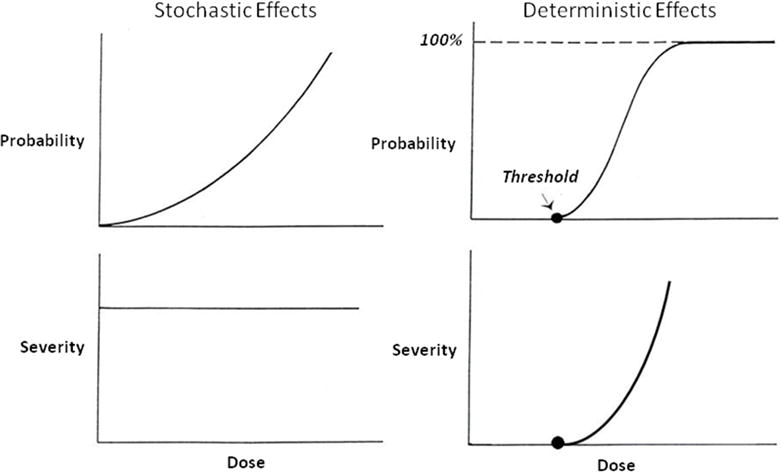
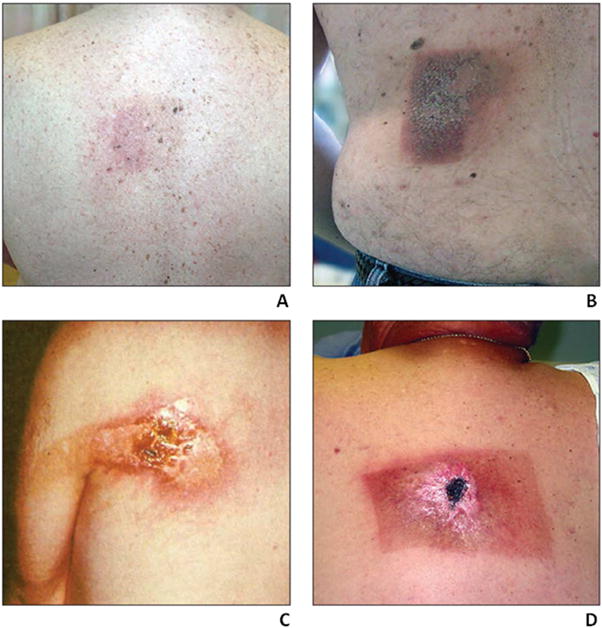
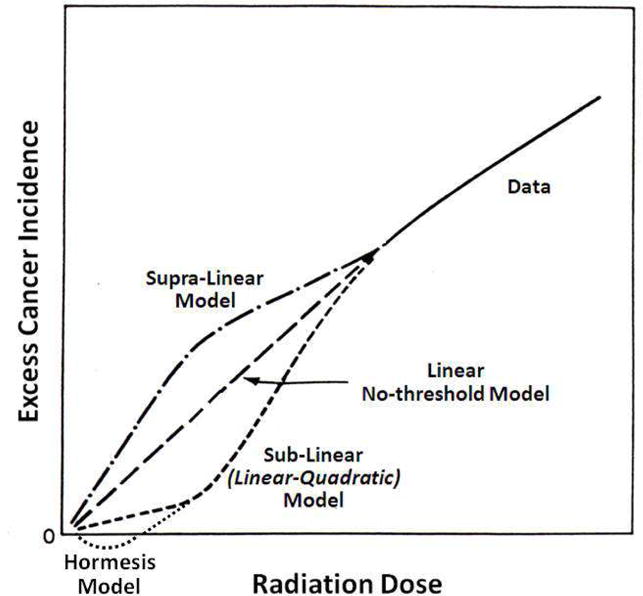
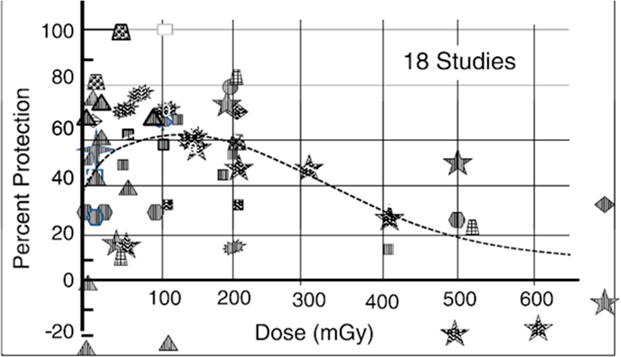
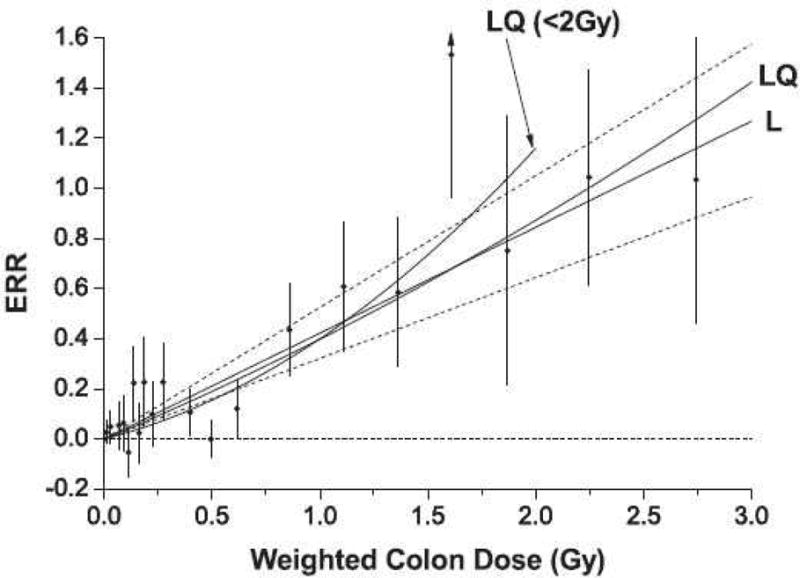
The introduction of ionizing radiation in medicine revolutionized the diagnosis and treatment of disease and dramatically improved and continues to improve the quality of health care. Cardiovascular imaging and medical imaging in general, however, are associated with a range of radiobiologic effects, including, in rare instances, moderate to severe skin damage resulting from cardiac fluoroscopy. For the dose range associated with diagnostic imaging (corresponding to effective doses on the order of 10 mSv [1 rem]), the possible effects are stochastic in nature and largely theoretical. The most notable of these effects, of course, is the possible increase in cancer risk. The current review addresses radiobiology relevant to cardiovascular imaging, with particular emphasis on radiation induction of cancer, including consideration of the linear nonthreshold dose-response model and of alternative models such as radiation hormesis.
Keywords: cancer risks; deterministic effects; hormesis; linear nonthreshold model; linear-quadratic model; radiation dosimetry; radiation effects; radiation genetic effects; radiobiology; reverse causation; stochastic effects.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ionizing Radiation NCRP. NCRP Report 160. Bethesda, MD: National Council on Radiation Protection and Measurements (NCRP); 2009. Exposure of the Population of the United States.
-
- Amis ES, Jr, Butler PF, Applegate KE, et al. American College of Radiology white paper on radiation dose in medicine. J Am Coll Radiol. 2007;4:272–84. - PubMed
-
- Redberg R, Smith-Bindman R. We are giving ourselves cancer. New York Times (Op-Ed) 2014
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
