

The histology of ovarian cancer: worldwide distribution and implications for international survival comparisons (CONCORD-2)
- PMID: 27931752
- PMCID: PMC6195192
- DOI: 10.1016/j.ygyno.2016.10.019
The histology of ovarian cancer: worldwide distribution and implications for international survival comparisons (CONCORD-2)
Erratum in
-
Erratum to "The histology of ovarian cancer: Worldwide distribution and implications for international survival comparisons (CONCORD-2)" [Gynecol. Oncol. 144 (2017) 405-413].Gynecol Oncol. 2017 Dec;147(3):726. doi: 10.1016/j.ygyno.2017.06.032. Epub 2017 Jul 5. Gynecol Oncol. 2017. PMID: 28687170 No abstract available.
Abstract
Objective: Ovarian cancers comprise several histologically distinct tumour groups with widely different prognosis. We aimed to describe the worldwide distribution of ovarian cancer histology and to understand what role this may play in international variation in survival.
Methods: The CONCORD programme is the largest population-based study of global trends in cancer survival. Data on 681,759 women diagnosed during 1995-2009 with cancer of the ovary, fallopian tube, peritoneum and retroperitonum in 51 countries were included. We categorised ovarian tumours into six histological groups, and explored the worldwide distribution of histology.
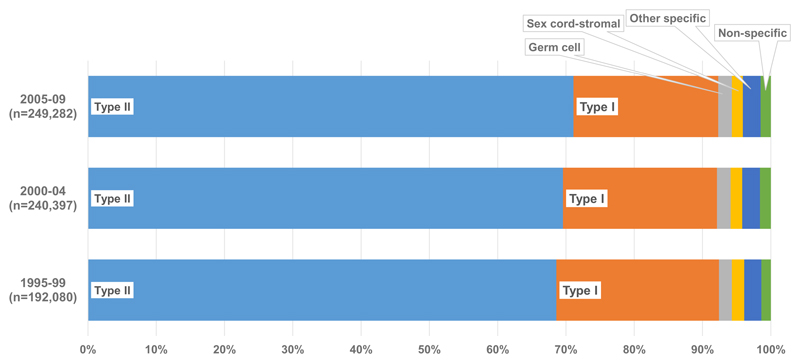
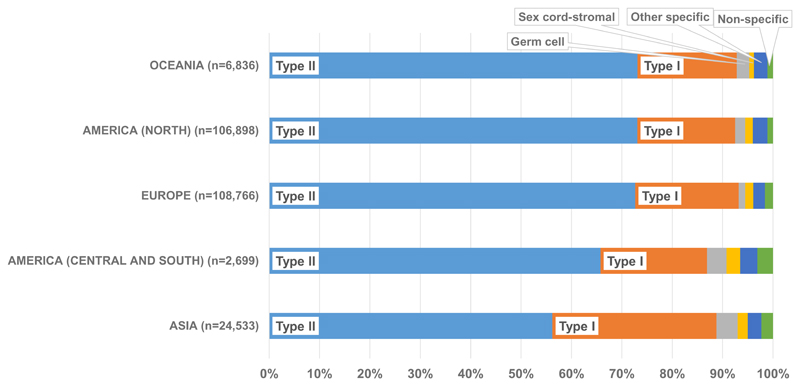
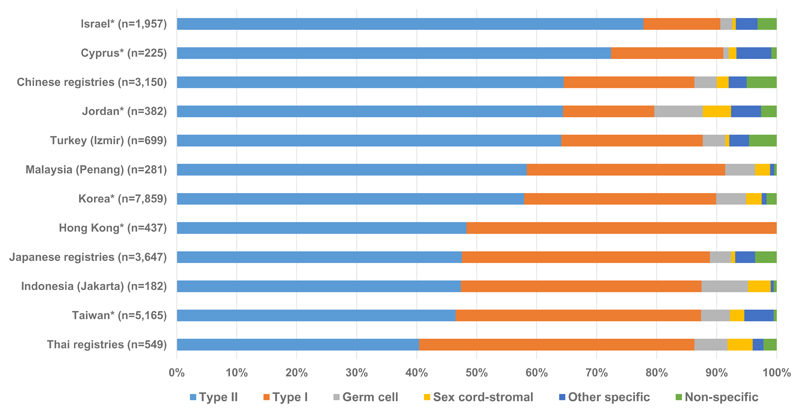
Results: During 2005-2009, type II epithelial tumours were the most common. The proportion was much higher in Oceania (73.1%), North America (73.0%) and Europe (72.6%) than in Central and South America (65.7%) and Asia (56.1%). By contrast, type I epithelial tumours were more common in Asia (32.5%), compared with only 19.4% in North America. From 1995 to 2009, the proportion of type II epithelial tumours increased from 68.6% to 71.1%, while the proportion of type I epithelial tumours fell from 23.8% to 21.2%. The proportions of germ cell tumours, sex cord-stromal tumours, other specific non-epithelial tumours and tumours of non-specific morphology all remained stable over time.
Conclusions: The distribution of ovarian cancer histology varies widely worldwide. Type I epithelial, germ cell and sex cord-stromal tumours are generally associated with higher survival than type II tumours, so the proportion of these tumours may influence survival estimates for all ovarian cancers combined. The distribution of histological groups should be considered when comparing survival between countries and regions.
Keywords: Epidemiology; Histology; Morphology; Ovarain cancer; Worldwide.
Copyright © 2016. Published by Elsevier Inc.
Conflict of interest statement
The authors declare there are no conflicts of interest.
Figures
References
-
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. Lyon, France: International Agency for Research on Cancer; 2013. [cited 2015 18 May]. [Internet]
-
- Kurman RJ, Carcangiu ML, Herrington CS, Young RH, editors. WHO Classification of Tumours of Female Reproductive Organs. 4th ed. Geneva: WHO; 2014.
-
- Maringe C, Walters S, Butler J, Coleman MP, Hacker N, Hanna L, et al. Stage at diagnosis and ovarian cancer survival: evidence from the International Cancer Benchmarking Partnership. Gynecologic Oncology. 2012;127:75–82. - PubMed
-
- Taylor H. Malignant and semi-malignant tumours of the ovary. Surg Gynecol Obsts. 1929(48):204–30.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
