

Mortality in the Hertfordshire Ageing Study: association with level and loss of hand grip strength in later life
- PMID: 27932364
- PMCID: PMC5500162
- DOI: 10.1093/ageing/afw222
Mortality in the Hertfordshire Ageing Study: association with level and loss of hand grip strength in later life
Abstract
Background: weak hand grip strength in later life is a risk factor for disability, morbidity and mortality and is central to definitions of sarcopenia and frailty. It is unclear whether rate of change in grip strength adds to level of grip strength as a risk factor for poor ageing outcomes.
Methods: study participants were 292 community-dwelling men and women whose grip strength was measured during the 1994/5 (average age 67) and 2003/5 (average age 76) phases of the Hertfordshire Ageing Study, UK. Individual rate of change in grip strength was estimated using a residual change method. Mortality was followed-up to 2011 (42 men and 21 women died).
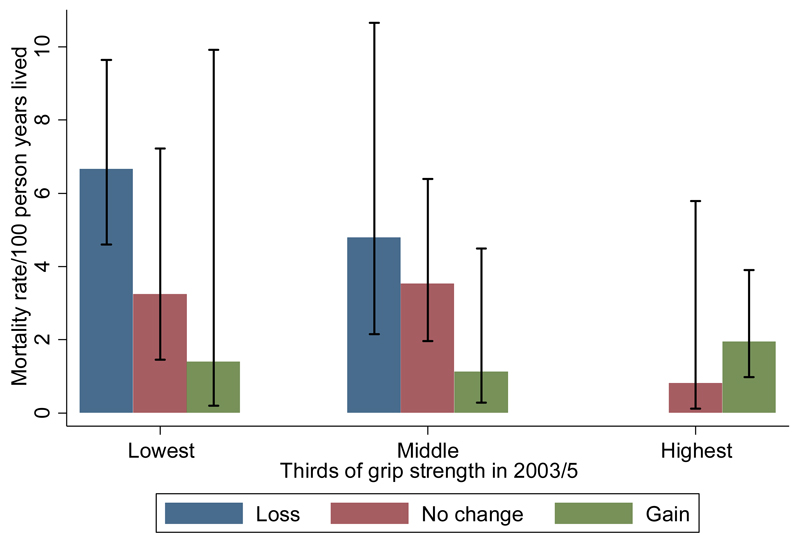
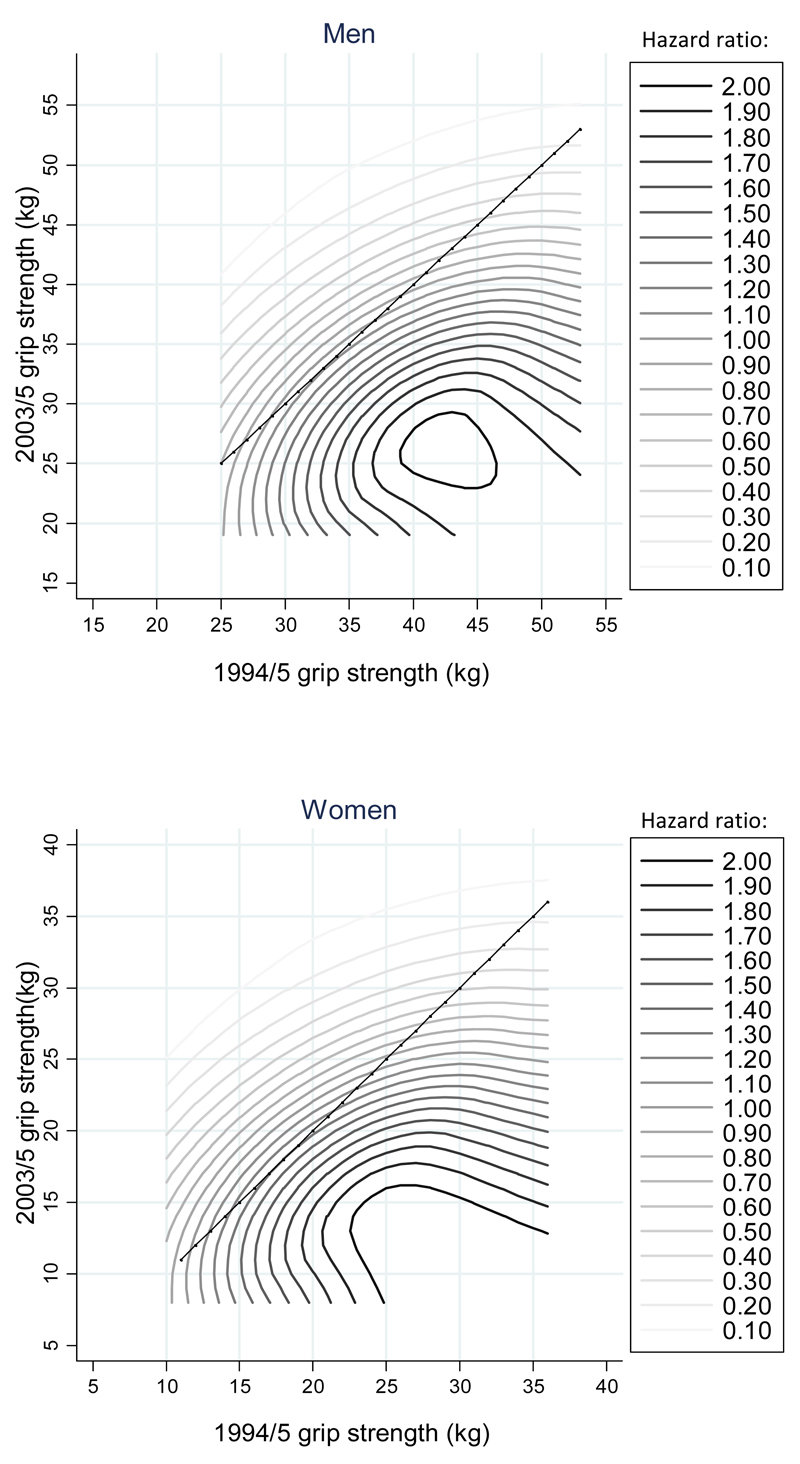
Results: average grip strengths in 2003/5 were 38.4 kg (standard deviation [SD] = 8.1) and 23.7 kg (SD = 6.6) for men and women respectively. Average annualised rates of change in grip strength (2003/5 minus 1994/5) were modest owing to a healthy-participant effect (men: -0.12 kg/y, SD = 0.71; women: 0.08 kg/y, SD = 0.54) but varied widely. Mortality risk varied according to level and rate of change in grip strength (P = 0.03); death rates per 100 person years of follow-up were 6.7 (95% CI: 4.6, 9.6) among participants who lost grip over time and had low grip in 2003/5, in contrast with 0.8 (95% CI: 0.1, 5.8) among participants whose grip changed little over time and remained high in 2003/5.
Conclusions: levels of grip strength in later life should be considered in conjunction with estimates of change in grip strength identified by repeat measurement over time. Normative data for longitudinal change in grip strength are required.
Keywords: change; epidemiology; longevity; older people; physical function; sarcopenia.
© The Author 2016. Published by Oxford University Press on behalf of the British Geriatrics Society. All rights reserved. For Permissions, please email: journals.permissions@oup.com
Conflict of interest statement
None declared.
Figures
Similar articles
-
Correlates of Level and Loss of Grip Strength in Later Life: Findings from the English Longitudinal Study of Ageing and the Hertfordshire Cohort Study.Calcif Tissue Int. 2018 Jan;102(1):53-63. doi: 10.1007/s00223-017-0337-5. Epub 2017 Oct 22. Calcif Tissue Int. 2018. PMID: 29058059 Free PMC article.
-
ACE inhibitors, statins and thiazides: no association with change in grip strength among community dwelling older men and women from the Hertfordshire Cohort Study.Age Ageing. 2014 Sep;43(5):661-6. doi: 10.1093/ageing/afu008. Epub 2014 Feb 11. Age Ageing. 2014. PMID: 24522120
-
Frailty or sarcopenia: which is a better indicator of mortality risk in older adults?J Epidemiol Community Health. 2025 Jan 13;79(2):124-130. doi: 10.1136/jech-2024-222678. J Epidemiol Community Health. 2025. PMID: 39393902 Free PMC article.
-
A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach.Age Ageing. 2011 Jul;40(4):423-9. doi: 10.1093/ageing/afr051. Epub 2011 May 30. Age Ageing. 2011. PMID: 21624928 Review.
-
Get a grip: individual variations in grip strength are a marker of brain health.Neurobiol Aging. 2018 Nov;71:189-222. doi: 10.1016/j.neurobiolaging.2018.07.023. Epub 2018 Aug 4. Neurobiol Aging. 2018. PMID: 30172220 Review.
Cited by
-
Terminal decline in objective and self-reported measures of motor function before death: 10 year follow-up of Whitehall II cohort study.BMJ. 2021 Aug 4;374:n1743. doi: 10.1136/bmj.n1743. BMJ. 2021. PMID: 34348957 Free PMC article.
-
An Inverse Relation between Hyperglycemia and Skeletal Muscle Mass Predicted by Using a Machine Learning Approach in Middle-Aged and Older Adults in Large Cohorts.J Clin Med. 2021 May 14;10(10):2133. doi: 10.3390/jcm10102133. J Clin Med. 2021. PMID: 34069247 Free PMC article.
-
Identification of Research Priorities in Exercise Oncology: A Consensus Study.J Cancer. 2020 Feb 19;11(9):2702-2707. doi: 10.7150/jca.42992. eCollection 2020. J Cancer. 2020. PMID: 32201540 Free PMC article.
-
Population-specific equations of age-related maximum handgrip force: a comprehensive review.PeerJ. 2024 Jul 22;12:e17703. doi: 10.7717/peerj.17703. eCollection 2024. PeerJ. 2024. PMID: 39056055 Free PMC article. Review.
-
Deep learning predicts all-cause mortality from longitudinal total-body DXA imaging.Commun Med (Lond). 2022 Aug 16;2:102. doi: 10.1038/s43856-022-00166-9. eCollection 2022. Commun Med (Lond). 2022. PMID: 35992891 Free PMC article.
References
MeSH terms
Grants and funding
- 19583/ARC_/Arthritis Research UK/United Kingdom
- MC_UP_A620_1015/MRC_/Medical Research Council/United Kingdom
- MC_U147574237/MRC_/Medical Research Council/United Kingdom
- MC_U147574234/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/2/MRC_/Medical Research Council/United Kingdom
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- MC_U147574212/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
