

Systematic review and quality analysis of emerging diagnostic measures for calcium pyrophosphate crystal deposition disease
- PMID: 27933211
- PMCID: PMC5133413
- DOI: 10.1136/rmdopen-2016-000339
Systematic review and quality analysis of emerging diagnostic measures for calcium pyrophosphate crystal deposition disease
Abstract
Objectives: Calcium pyrophosphate crystal deposition disease (CPPD) is common, yet prevalence and overall clinical impact remain unclear. Sensitivity and specificity of CPPD reference standards (conventional crystal analysis (CCA) and radiography (CR)) were meta-analysed by EULAR (published 2011). Since then, new diagnostic modalities are emerging. Hence, we updated 2009-2016 literature findings by systematic review and evidence grading, and assessed unmet needs.
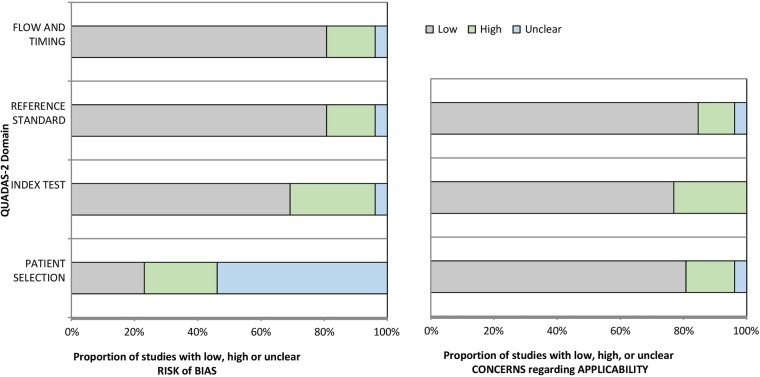
Methods: We performed systematic search of full papers (PubMed, Scopus/EMBASE, Cochrane 2009-2016 databases). Search terms included CPPD, chondrocalcinosis, pseudogout, ultrasound, MRI, dual energy CT (DECT). Paper selection, data abstraction, EULAR evidence level, and Quality Assessment of Diagnostic Accuracy Studies (QUADAS)-2 bias and applicability grading were performed independently by 3 authors.
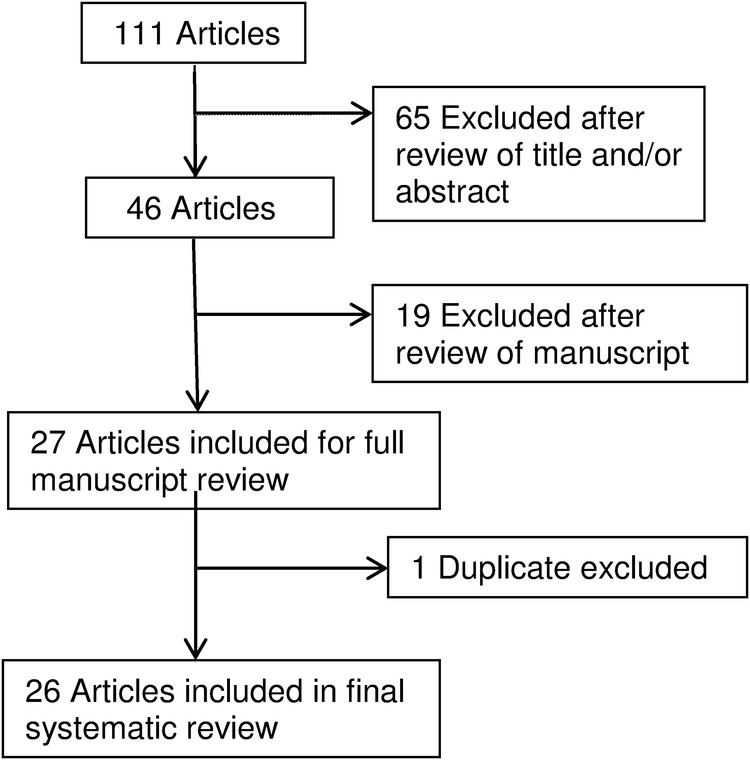
Results: We included 26 of 111 eligible papers, which showed emergence in CPPD diagnosis of ultrasound (U/S), and to lesser degree, DECT and Raman spectroscopy. U/S detected CPPD crystals in peripheral joints with sensitivity >80%, superior to CR. However, most study designs, though analytical, yielded low EULAR evidence level. DECT was marginally explored for CPPD, compared with 35 published DECT studies in gout. QUADAS-2 grading indicated strong applicability of U/S, DECT and Raman spectroscopy, but high study bias risk (in ∼30% of papers) due to non-controlled designs, and non-randomised subject selection.
Conclusions: Though CCA and CR remain reference standards for CPPD diagnosis, U/S, DECT and Raman spectroscopy are emerging U/S sensitivity appears to be superior to CR. We identified major unmet needs, including for randomised, blinded, controlled studies of CPPD diagnostic performance and rigorous analyses of 4 T MRI and other emerging modalities.
Keywords: Chondrocalcinosis; Qualitative research; Quality Indicators; Synovial fluid; Ultrasonography.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Terkeltaub R. Calcium crystal disease. Calcium pyrophosphate dihydrate and basic calcium phosphate: Epidemiology. In: Firestein GS, Budd RC, Gabriel SE, McInnes IB, O'Dell JR, eds Kelley's textbook of rheumatology. 9th edn Philadelphia: Elsevier Saunders, 2012;1576–7.
LinkOut - more resources
Full Text Sources
Other Literature Sources