

Clinical analysis on 430 cases of infantile purulent meningitis
- PMID: 27933250
- PMCID: PMC5118376
- DOI: 10.1186/s40064-016-3673-4
Clinical analysis on 430 cases of infantile purulent meningitis
Abstract
Background: Purulent meningitis (PM) usually caused by a variety of pyogenic infection, is a kind of central nervous system infectious disease mostly common in children. It is easily misdiagnosed and its symptoms are varied. Excessive application of broad-spectrum antibiotics results in increased sickness and death of infants and young children. In this study, clinical data of 430 cases of PM in infants were analyzed to summarize the clinical experiences so as to achieve early diagnosis and early treatment of PM.
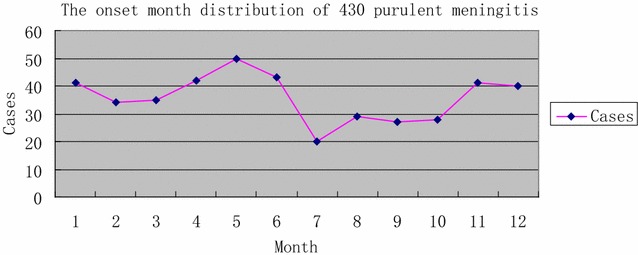
Results: Male-to-female ratio was 1.61:1, and the median age of incidence was 0.42 years. May was the modal month of onset (11.7%). Main clinical manifestations were fever (89.3%), vomiting (67.2%), mental fatigue (62.1%), anterior fontanelle full/bulging/high tension (54.2%), convulsion (52.6%), and meningeal irritation sign (24.7%). Cerebrospinal fluid (CSF) bacterial culture was done for 420 cases, of which 1.2% cases were positive. Blood culture was done for 146 cases of which 15.1% were positive. 175 (40.7%) cases had complications, among which 133 cases (76.0%) were subdural effusion, 21 cases (12.0%) were epilepsy.
Conclusion: Infantile PM is common in Spring, and May is the modal month of onset. The CSF/blood pathogen detection rate is very low and it is difficult to find evidence of cause. Fever, vomiting, mental fatigue and anterior fontanelle full/bulging/high tension, convulsion are the main clinical manifestations on which diagnosis depends. For those children diagnosed as PM and still having recurrent fever and prominent anterior fontanelle after treatment, clinicians should consider the probability of subdural effusion and treat them with brain imaging test on time.
Keywords: Clinical manifestation; Diagnosis; Infantile purulent meningitis.
Figures
Similar articles
-
[A multicentric clinical study on clinical characteristics and drug sensitivity of children with pneumococcal meningitis in China].Zhonghua Er Ke Za Zhi. 2019 May 2;57(5):355-362. doi: 10.3760/cma.j.issn.0578-1310.2019.05.008. Zhonghua Er Ke Za Zhi. 2019. PMID: 31060128 Chinese.
-
[Clinical analysis of purulent meningitis in 317 children].Zhongguo Dang Dai Er Ke Za Zhi. 2015 Jul;17(7):710-4. Zhongguo Dang Dai Er Ke Za Zhi. 2015. PMID: 26182277 Chinese.
-
[A multicenter epidemiological study of neonatal bacterial meningitis in parts of South China].Zhonghua Er Ke Za Zhi. 2018 Jun 2;56(6):421-428. doi: 10.3760/cma.j.issn.0578-1310.2018.06.004. Zhonghua Er Ke Za Zhi. 2018. PMID: 29886604 Chinese.
-
Subdural empyema in children.Childs Nerv Syst. 2018 Oct;34(10):1881-1887. doi: 10.1007/s00381-018-3907-6. Epub 2018 Jul 16. Childs Nerv Syst. 2018. PMID: 30014307 Review.
-
[Meningitis (I)--differential diagnosis; aseptic and chronic meningitis].Ther Umsch. 1999 Nov;56(11):631-9. doi: 10.1024/0040-5930.56.11.631. Ther Umsch. 1999. PMID: 10596275 Review. German.
Cited by
-
Reappraisal of the Optimal Dose of Meropenem in Critically Ill Infants and Children: a Developmental Pharmacokinetic-Pharmacodynamic Analysis.Antimicrob Agents Chemother. 2020 Jul 22;64(8):e00760-20. doi: 10.1128/AAC.00760-20. Print 2020 Jul 22. Antimicrob Agents Chemother. 2020. PMID: 32513801 Free PMC article.
-
Clinical manifestations and laboratory results of 61 children with infectious mononucleosis.J Int Med Res. 2020 Oct;48(10):300060520924550. doi: 10.1177/0300060520924550. J Int Med Res. 2020. PMID: 33045888 Free PMC article.
-
Factors Predictive of Varicella Zoster Virus Encephalitis/Meningitis: A Single-Center, Retrospective Study.Med Sci Monit. 2022 Sep 28;28:e938057. doi: 10.12659/MSM.938057. Med Sci Monit. 2022. PMID: 36168237 Free PMC article.
-
Main Clinical and Laboratory Features of Children with Bacterial Meningitis: Experience from a Tertiary Paediatric Centre in Central Vietnam.Pediatric Health Med Ther. 2022 Aug 26;13:289-295. doi: 10.2147/PHMT.S371914. eCollection 2022. Pediatric Health Med Ther. 2022. PMID: 36051354 Free PMC article.
-
Ameliorative effects of ceftriaxone sodium combined with dexamethasone on infantile purulent meningitis and associated effects on brain-derived neurotrophic factor levels.Exp Ther Med. 2020 Aug;20(2):945-951. doi: 10.3892/etm.2020.8769. Epub 2020 May 19. Exp Ther Med. 2020. PMID: 32742338 Free PMC article.
References
-
- Carroll KJ, Carroll C. A prospective investigation of the long-term auditory-neurological sequelae associated with bacterial meningitis: a study from Vanuatu. J Trop Med Hyg. 1994;97:145–150. - PubMed
-
- Deasy J. The antibiotic challenge: changing clinical management of infections. JAAPA. 2009;22:22–26. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
