

Second malignancies in the context of lenalidomide treatment: an analysis of 2732 myeloma patients enrolled to the Myeloma XI trial
- PMID: 27935580
- PMCID: PMC5223149
- DOI: 10.1038/bcj.2016.114
Second malignancies in the context of lenalidomide treatment: an analysis of 2732 myeloma patients enrolled to the Myeloma XI trial
Abstract
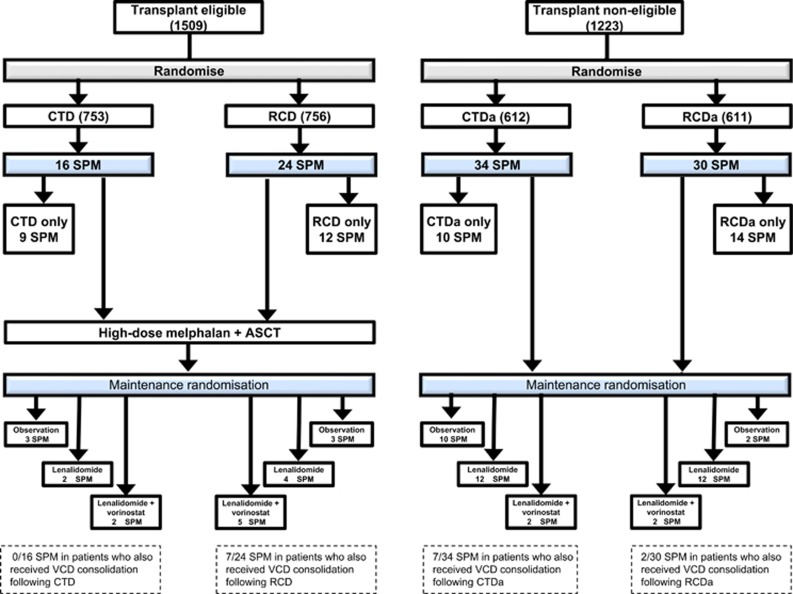
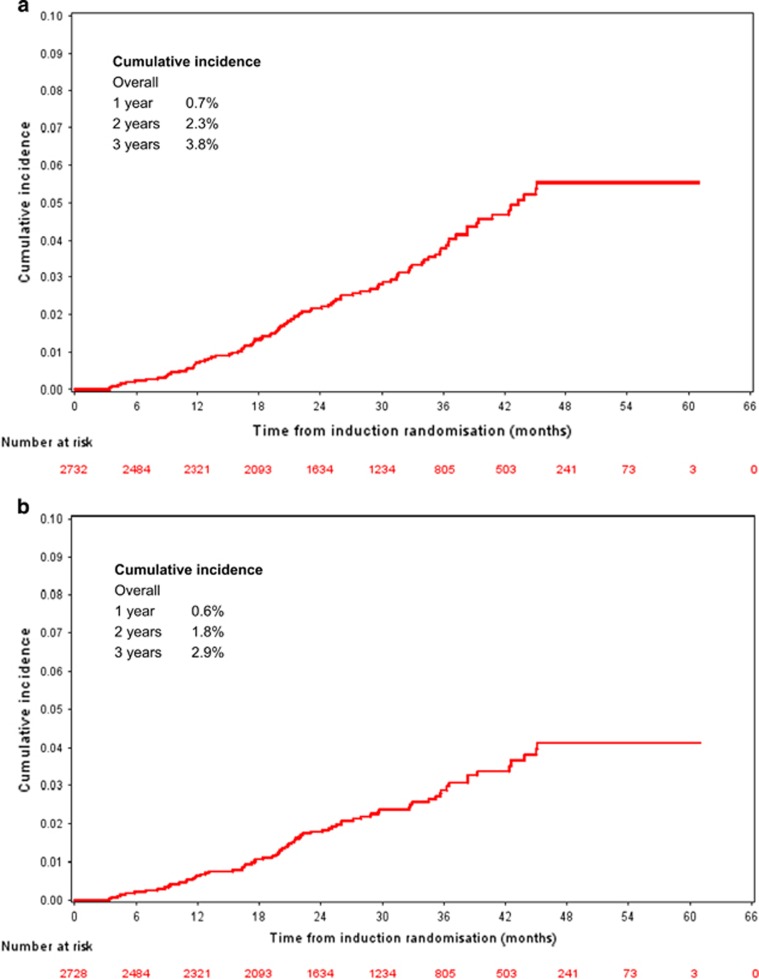
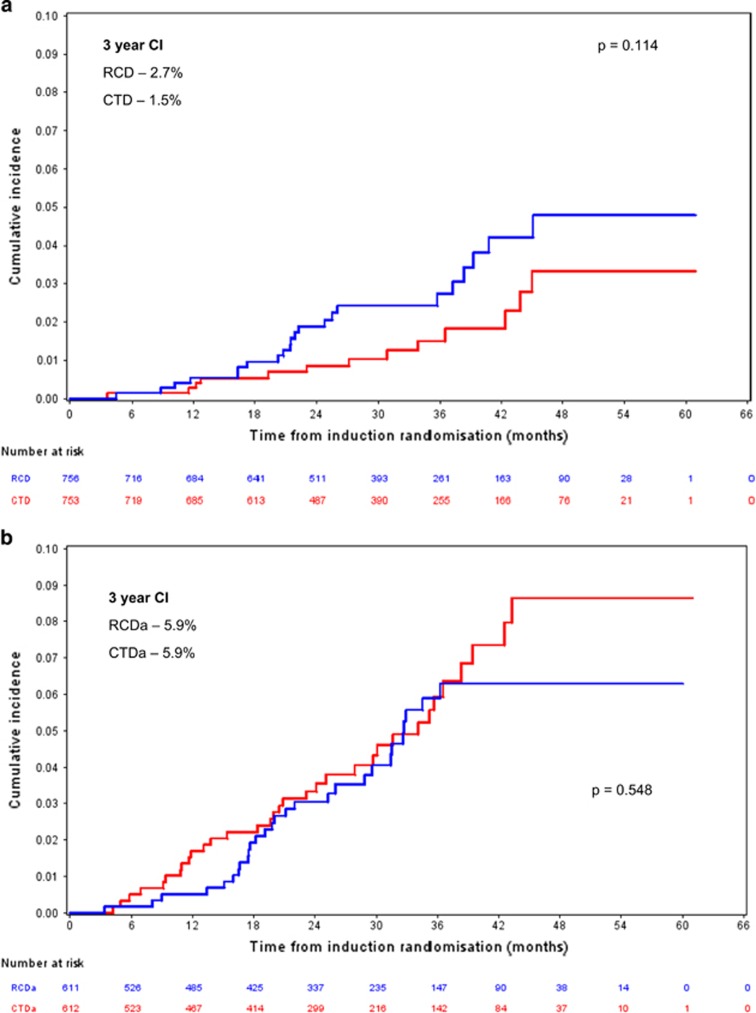
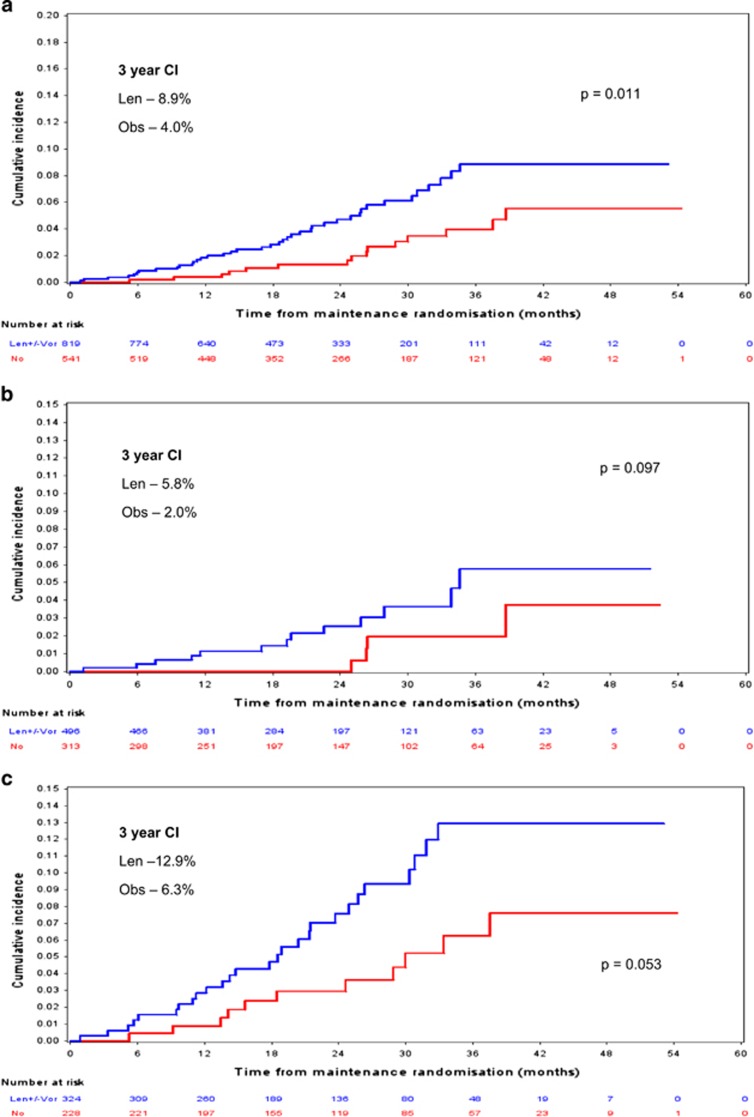
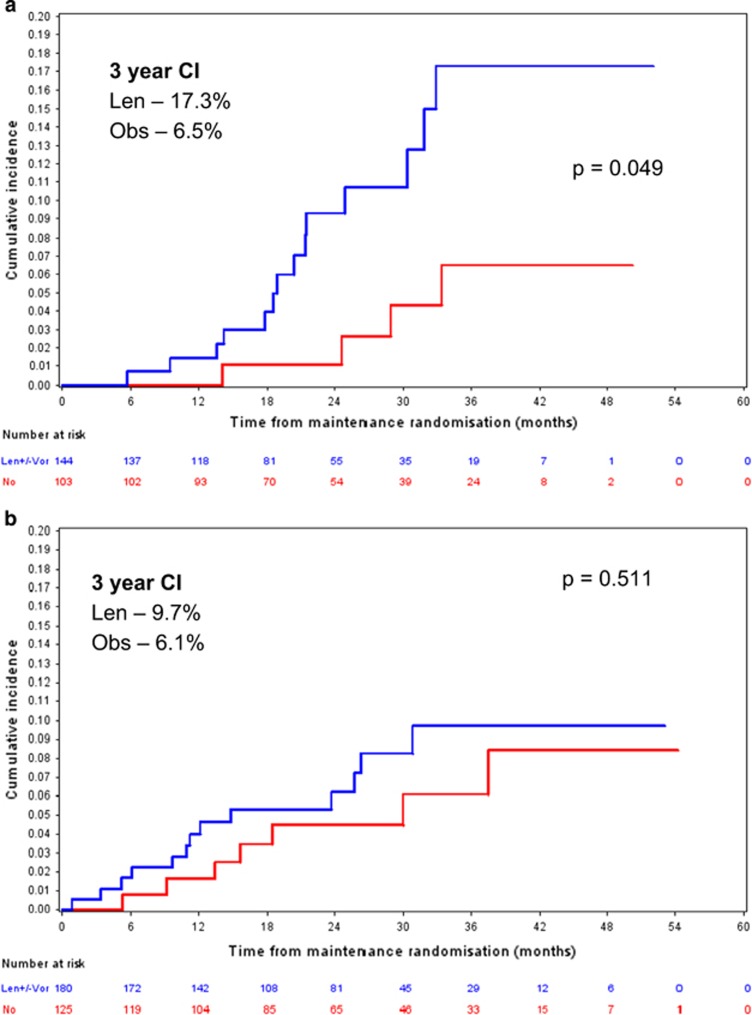
We have carried out the largest randomised trial to date of newly diagnosed myeloma patients, in which lenalidomide has been used as an induction and maintenance treatment option and here report its impact on second primary malignancy (SPM) incidence and pathology. After review, 104 SPMs were confirmed in 96 of 2732 trial patients. The cumulative incidence of SPM was 0.7% (95% confidence interval (CI) 0.4-1.0%), 2.3% (95% CI 1.6-2.7%) and 3.8% (95% CI 2.9-4.6%) at 1, 2 and 3 years, respectively. Patients receiving maintenance lenalidomide had a significantly higher SPM incidence overall (P=0.011). Age is a risk factor with the highest SPM incidence observed in transplant non-eligible patients aged >74 years receiving lenalidomide maintenance. The 3-year cumulative incidence in this group was 17.3% (95% CI 8.2-26.4%), compared with 6.5% (95% CI 0.2-12.9%) in observation only patients (P=0.049). There was a low overall incidence of haematological SPM (0.5%). The higher SPM incidence in patients receiving lenalidomide maintenance therapy, especially in advanced age, warrants ongoing monitoring although the benefit on survival is likely to outweigh risk.
Conflict of interest statement
JRJ has received research and travel support from Celgene; WG: honoraria from Janssen and Celgene; CP: advisory board, honoraria and travel support from Celgene, Novartis and Takeda; MK: honoraria, consultancy, research funding and travel support from Celgene, BristolMyerSquibb (BMS), Chugia, Janssen and Takeda; MJ: honoraria from Takeda and Janssen; GC: consultancy and research funding from Janssen, Celgene, Takeda Oncology, Sanofi, Amgen and BMS; GP: Celgene Honoraria; BK: Celgene and Jazz Pharmaceuticals; FD: honoraria and travel support from Takeda-Milenium, Onyx-Amgen, Celgene and Janssen; KB: honoraria and travel support from Celgene and Janssen; RGO: honoraria and research funding from Celgene and Janssen; GHJ: honoraria from Celgene, Takeda and Amgen; GJM: honoraria, advisory committee, research funding; CancerNet, Multiple Myeloma Research Foundation, Celgene, Takeda-Millennium, BMS and Weisman Institute. The remaining authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
