

doi: 10.1167/iovs.16-21031.
Diabetic Retinopathy: Battling the Global Epidemic
Affiliations
- PMID: 27936469
- PMCID: PMC5152562
- DOI: 10.1167/iovs.16-21031
Item in Clipboard
Diabetic Retinopathy: Battling the Global Epidemic
Invest Ophthalmol Vis Sci.
.
No abstract available
Figures
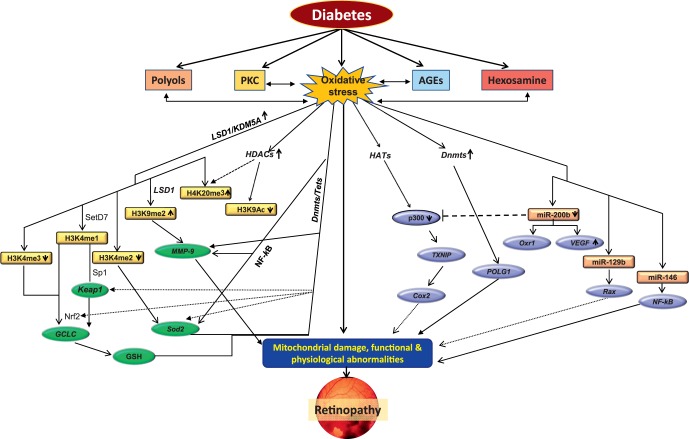
Metabolic abnormalities and epigenetic modifications in diabetic retinopathy. Circulating high glucose increases oxidative stress and alters many metabolic pathways, including increased production of polyols and advanced glycation end products (AGEs), and activates protein kinase C (PKC) and hexosamine pathways. These metabolic pathways, in addition to increasing oxidative stress, are also activated by oxidative stress. Increased oxidative stress damages mitochondria, and damaged mitochondria themselves further fuel into oxidative stress. Enzymes responsible for epigenetic modifications, including for maintaining histone acetylation (HATs and HDACs) and methylation (SetD7 and LSD1) and DNA methylation/hydroxyl-methylation (Dnmts/Tets), are altered, affecting histone modifications and/or DNA methylation in the promoter regions of many genes associated with the development of diabetic retinopathy. Alteration in the transcription of the genes associated with oxidative stress, including Sod2, GCLC, MMP-9, and POLG (gene encoding mitochondrial superoxide dismutase, glutamyl cysteine synthase, matrix metalloproteinase-9, and polymerase gamma for mtDNA biogenesis, respectively), further compromises mitochondrial homeostasis. In addition, many microRNAs (e.g., miR 200b, miR 129b, and miR 146) are also altered, fueling into mitochondrial damage. Damaged mitochondria accelerate capillary cell apoptosis, resulting in cell loss and the development of diabetic retinopathy. By courtesy of Renu Kowluru, PhD.
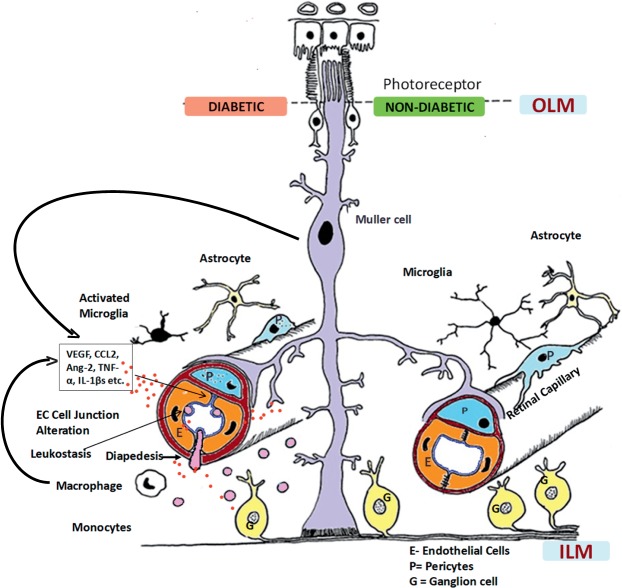
Neurovascular unit of the retina in nondiabetic and diabetic conditions. Normally, pericytes and endothelial cells constitute the blood–retinal barrier (BRB) (retinal capillary) that is covered intimately by multiple processes of the Müller cells (right). Astrocytes and microglia with long processes also surround the capillaries, maintaining the normal homeostasis for neuronal signaling and synaptic transmission. In diabetes, chronic inflammation sets in, contributing to the breakdown of the BRB (left). Müller cells and endothelial cells produce chemokines (including monocyte chemoattractant protein-1) that lead to increased leukostasis, diapedesis, and influx of monocytes into the retina and increased production of cytokines, including vascular endothelial growth factor (VEGF), tumor necrosis factor (TNF)α, interleukin (IL)-1β, matrix metalloproteinase, and angiopoietin (Ang)-2. These inflammatory mediators then result in the breakdown of endothelial cell–cell junctions. Microglia become activated, and there is increased apoptosis of ganglion cells and amacrine cells, which deranges synaptic degeneration. In retinal capillaries, pericyte dropout and thickening of the basement membrane also occur as a result of hyperglycemia, all contributing to increased leakage from vessels. Photoreceptors contribute to production of superoxide and inflammatory proteins in this process. CCL-2, chemokine ligand 2; EC, endothelial cell; ILM, inner limiting membrane; OLM, outer limiting membrane. Reprinted with permission from Das A, McGuire PG, Rangasamy S. Diabetic Macular Edema: Pathophysiology and Novel Therapeutic Targets. Ophthalmology. 2015;122:1375–1394. Copyright © 2015 American Academy of Ophthalmology. Published by Elsevier, Inc. All rights reserved.
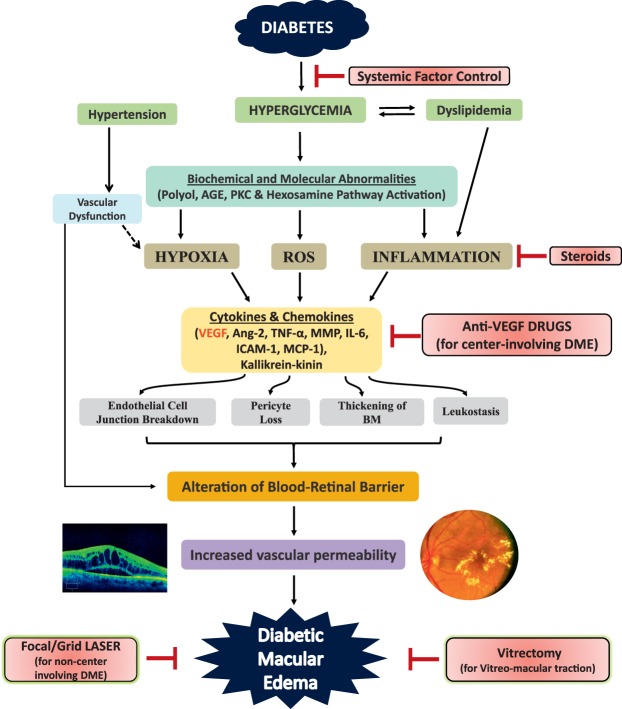
Pathophysiology of diabetic macular edema (DME) and different therapeutic strategies. Hyperglycemia in diabetes activates different biochemical pathways that lead to increased hypoxia, reactive oxygen species (ROS) formation, and inflammation with production of cytokines and chemokines. These mediators then cause endothelial cell junction breakdown and leukostasis, resulting in alteration of the blood–retinal barrier (BRB), increased retinal vascular permeability, and DME. Hyperglycemia also causes thickening of the basement membrane (BM) and pericyte dropout. Hypertension and hyperlipidemia, which coexist commonly in diabetic persons, further damage the already altered BRB. Currently, control of systemic factors, focal/grid laser (for noncenter-involving DME), anti-vascular endothelial growth factor (VEGF) therapies (for center-involving DME), steroids, and vitrectomy (in cases of vitreomacular traction) are the mainstays of management of DME. However, the current anti-VEGF therapies have limitations because they target only VEGF rather than other inflammatory molecules (e.g., angiopoietin [Ang]-2, matrix metalloproteinase [MMP], tumor necrosis factor [TNF]α, interleukin [IL]-1β, kallikrein–kinin) present in the retina in diabetic persons. Many future therapies target these other mediators. AGE, advanced glycation end products; ICAM, intercellular adhesion molecule; MCP, monocyte chemoattractant protein; PKC, protein kinase C. Reprinted with permission from Das A, McGuire PG, Rangasamy S. Diabetic Macular Edema: Pathophysiology and Novel Therapeutic Targets. Ophthalmology. 2015;122:1375–1394. Copyright © 2015 American Academy of Ophthalmology. Published by Elsevier, Inc. All rights reserved.
References
-
- International Diabetes Federation. IDF Diabetes Atlas. 7th ed. Brussels, Belgium: International Diabetes Federation; 2015.
-
- Huang OS,, Tay WT,, Tai ES,, et al. Lack of awareness amongst community patients with diabetes and diabetic retinopathy: the Singapore Malay Eye Study. Ann Acad Med Singapore. 2009; 38: 1048–1055. - PubMed
-
- Anjana RM, Shanthi Rani CS,, Deepa M,, et al. Incidence of diabetes and prediabetes and predictors of progression among Asian Indians: 10-year follow-up of the Chennai Urban Rural Epidemiology Study (CURES). Diabetes Care. 2015; 38: 1441–1448. - PubMed
-
- Raman R,, Rani PK,, Gnanamoorthy P,, et al. Association of obesity with diabetic retinopathy: Sankara Nethralaya Diabetic Retinopathy Epidemiology and Molecular Genetics Study (SN-DREAMS Report no. 8). Acta Diabetol. 2010; 47: 209–215. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
