

Effects of Physician-targeted Pay for Performance on Use of Spontaneous Breathing Trials in Mechanically Ventilated Patients
- PMID: 27936874
- PMCID: PMC5519961
- DOI: 10.1164/rccm.201607-1505OC
Effects of Physician-targeted Pay for Performance on Use of Spontaneous Breathing Trials in Mechanically Ventilated Patients
Abstract
Rationale: Pay for performance is an increasingly common quality improvement strategy despite the absence of robust supporting evidence.
Objectives: To determine the impact of a financial incentive program rewarding physicians for the completion of daily spontaneous breathing trials (SBTs) in three academic hospitals.
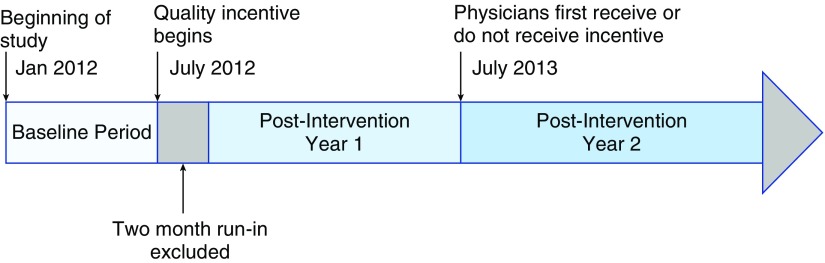
Methods: We compared data from mechanically ventilated patients from 6 months before to 2 years after introduction of a financial incentive program that provided annual payments to critical care physicians contingent on unit-level SBT completion rates. We used Poisson regression to compare the frequency of days on which SBTs were completed among eligible patients and days on which patients were excluded from SBT eligibility among all mechanically ventilated patients. We used multivariate regression to compare risk-adjusted duration of mechanical ventilation and in-hospital mortality.
Measurements and main results: The cohort included 7,291 mechanically ventilated patients with 75,621 ventilator days. Baseline daily SBT rates were 96.8% (hospital A), 16.4% (hospital B), and 74.7% (hospital C). In hospital A, with the best baseline performance, there was no change in SBT rates, exclusion rates, or duration of mechanical ventilation across time periods. In hospitals B and C, with lower SBT completion rates at baseline, there was an increase in daily SBT completion rates and a concomitant increase in exclusions from eligibility. Duration of mechanical ventilation decreased in hospital C but not in hospital B. Mortality was unchanged for all hospitals.
Conclusions: In hospitals with low baseline SBT completion, physician-targeted financial incentives were associated with increased SBT rates driven in part by increased exclusion rates, without consistent improvements in outcome.
Keywords: critical care; health care quality; mechanical ventilation; pay for performance.
Figures


Comment in
-
Changing Intensivists' Behaviors: A Challenge in Need of New Solutions.Am J Respir Crit Care Med. 2017 Jul 1;196(1):2-4. doi: 10.1164/rccm.201701-0020ED. Am J Respir Crit Care Med. 2017. PMID: 28665202 Free PMC article. No abstract available.
References
-
- Esteban A, Frutos F, Tobin MJ, Alía I, Solsona JF, Valverdú I, Fernández R, de la Cal MA, Benito S, Tomás R, et al. Spanish Lung Failure Collaborative Group. A comparison of four methods of weaning patients from mechanical ventilation. N Engl J Med. 1995;332:345–350. - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, et al. Surviving Sepsis Campaign Guidelines Committee Including the Pediatric Subgroup. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637. - PubMed
-
- MacIntyre NR, Cook DJ, Ely EW, Jr, Epstein SK, Fink JB, Heffner JE, Hess D, Hubmayer RD, Scheinhorn DJ American College of Chest Physicians; American Association for Respiratory Care; American College of Critical Care Medicine. Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest. 2001;120(6, Suppl):375S–395S. - PubMed
-
- Robertson TE, Mann HJ, Hyzy R, Rogers A, Douglas I, Waxman AB, Weinert C, Alapat P, Guntupalli KK, Buchman TG Partnership for Excellence in Critical Care. Multicenter implementation of a consensus-developed, evidence-based, spontaneous breathing trial protocol. Crit Care Med. 2008;36:2753–2762. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
