

Minimal Change Disease
- PMID: 27940460
- PMCID: PMC5293332
- DOI: 10.2215/CJN.05000516
Minimal Change Disease
Abstract
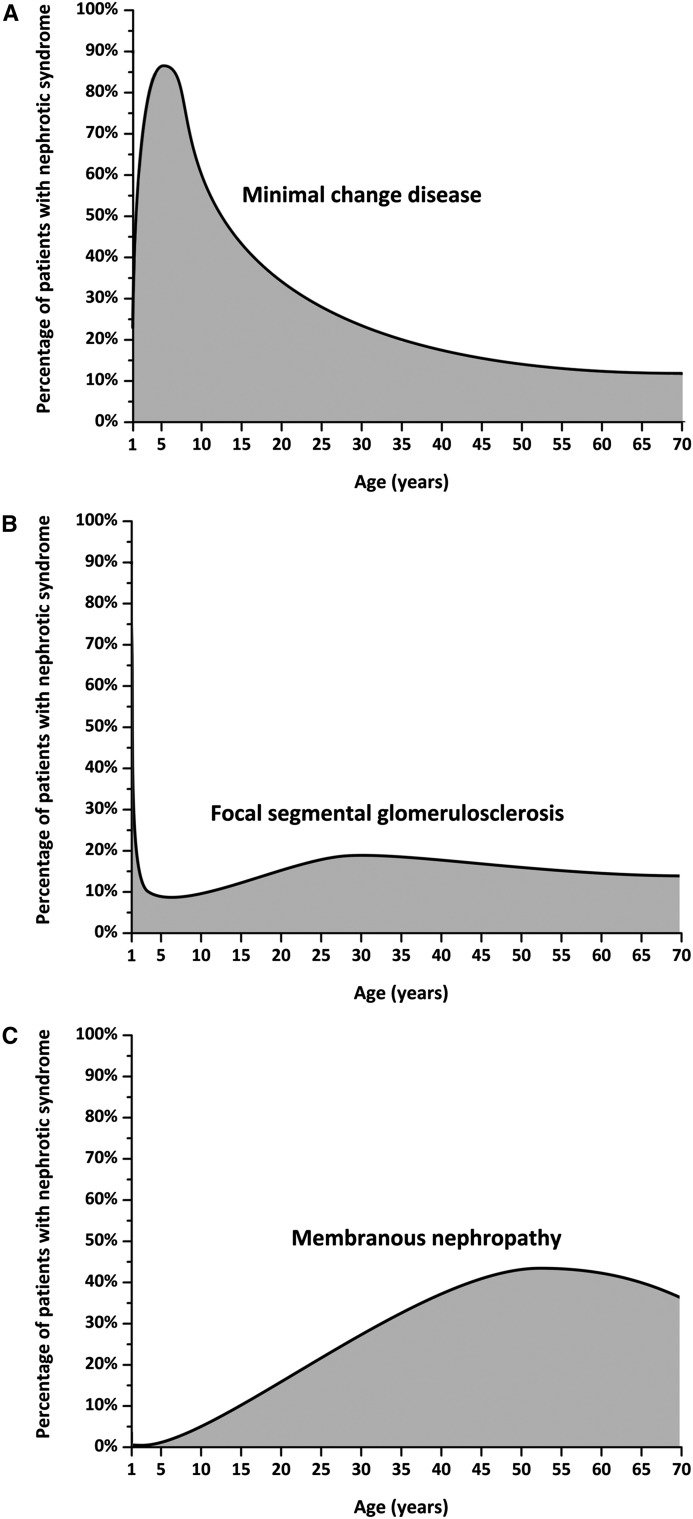
Minimal change disease (MCD) is a major cause of idiopathic nephrotic syndrome (NS), characterized by intense proteinuria leading to edema and intravascular volume depletion. In adults, it accounts for approximately 15% of patients with idiopathic NS, reaching a much higher percentage at younger ages, up to 70%-90% in children >1 year of age. In the pediatric setting, a renal biopsy is usually not performed if presentation is typical and the patient responds to therapy with oral prednisone at conventional doses. Therefore, in this setting steroid-sensitive NS can be considered synonymous with MCD. The pathologic hallmark of disease is absence of visible alterations by light microscopy and effacement of foot processes by electron microscopy. Although the cause is unknown and it is likely that different subgroups of disease recognize a different pathogenesis, immunologic dysregulation and modifications of the podocyte are thought to synergize in altering the integrity of the glomerular basement membrane and therefore determining proteinuria. The mainstay of therapy is prednisone, but steroid-sensitive forms frequently relapse and this leads to a percentage of patients requiring second-line steroid-sparing immunosuppression. The outcome is variable, but forms of MCD that respond to steroids usually do not lead to chronic renal damage, whereas forms that are unresponsive to steroids may subsequently reveal themselves as FSGS. However, in a substantial number of patients the disease is recurrent and requires long-term immunosuppression, with significant morbidity because of side effects. Recent therapeutic advances, such as the use of anti-CD20 antibodies, have provided long-term remission off-therapy and suggest new hypotheses for disease pathogenesis.
Keywords: nephrotic syndrome; pathology; pediatric nephrology; podocyte; proteinuria; renal.
Copyright © 2017 by the American Society of Nephrology.
Figures

References
-
- Nachman PH, Jennette JC, Falk RJ: Primary glomerular disease. In: The Kidney, 8th Ed., edited by Brenner BM, Philadelphia, Saunders Elsevier, 2008, pp 987–1066
-
- Cameron JS: The nephrotic syndrome and its complications. Am J Kidney Dis 10: 157–171, 1987 - PubMed
-
- Eddy AA, Symons JM: Nephrotic syndrome in childhood. Lancet 362: 629–639, 2003 - PubMed
-
- Floege J, Amann K: Primary glomerulonephritides. Lancet 387: 2036–2048, 2016 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
