

Endovascular treatment improves cognition after stroke: A secondary analysis of REVASCAT trial
- PMID: 27940648
- PMCID: PMC5272792
- DOI: 10.1212/WNL.0000000000003517
Endovascular treatment improves cognition after stroke: A secondary analysis of REVASCAT trial
Abstract
Objective: To investigate the effect of endovascular treatment on cognitive function as a prespecified secondary analysis of the REVASCAT (Endovascular Revascularization With Solitaire Device Versus Best Medical Therapy in Anterior Circulation Stroke Within 8 Hours) trial.
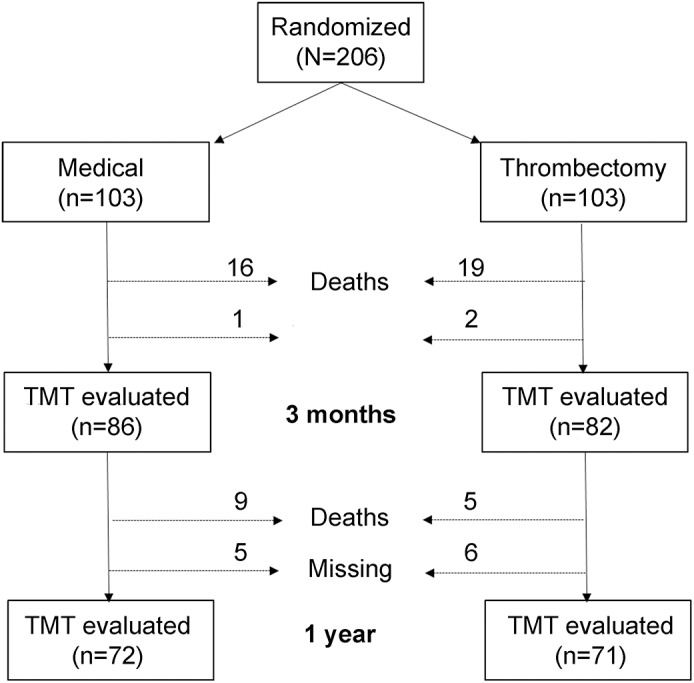
Methods: REVASCAT randomized 206 patients with anterior circulation proximal arterial occlusion stroke to Solitaire thrombectomy or best medical treatment alone. Patients with established dementia were excluded from enrollment. Cognitive function was assessed in person with Trail Making Test (TMT) Parts A and B at 3 months and 1 year after randomization by an investigator masked to treatment allocation. Test completion within 5 minutes, time of completion (seconds), and number of errors were recorded.
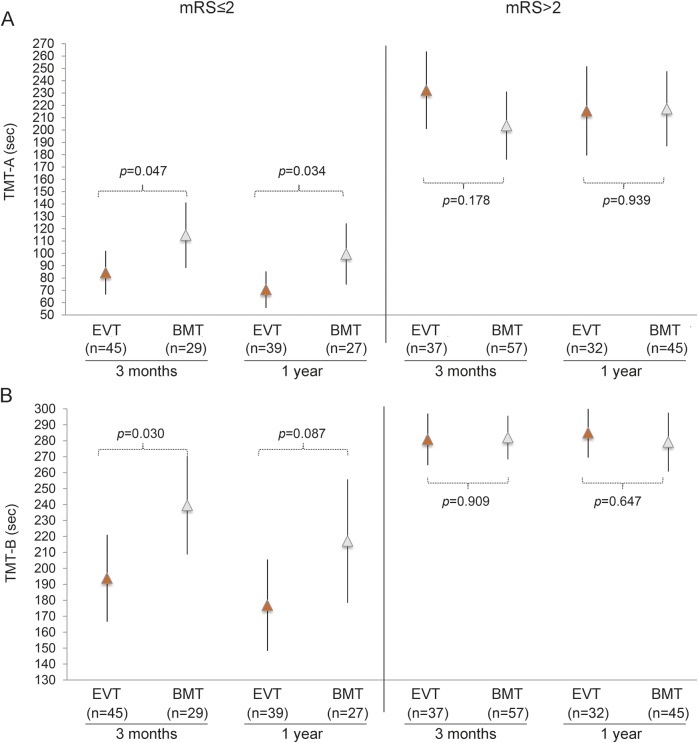
Results: From November 2012 to December 2014, 206 patients were enrolled in REVASCAT. TMT was assessed in 82 of 84 patients undergoing thrombectomy and 86 of 87 control patients alive at 3 months and in 71 of 79 patients undergoing thrombectomy and 72 of 78 control patients alive at 1 year. Rates of timely TMT-A completion were similar in both treatment arms, although patients undergoing thrombectomy required less time for TMT-A completion and had higher rates of error-free TMT-A performance. Thrombectomy was also associated with a higher probability of timely TMT-B completion (adjusted odds ratio 3.17, 95% confidence interval 1.51-6.66 at 3 months; and adjusted ratio 3.66, 95% confidence interval 1.60-8.35 at 1 year) and shorter time for TMT-B completion. Differences in TMT completion times between treatment arms were significant in patients with good functional outcome but not in those who were functionally dependent (modified Rankin Scale score >2). Poorer cognitive outcomes were significantly associated with larger infarct volume, higher modified Rankin Scale scores, and worse quality of life.
Conclusions: Thrombectomy improves TMT performance after stroke, especially among patients who reach good functional recovery.
Clinicaltrialsgov identifier: NCT01692379.
Classification of evidence: This study provides Class I evidence that for patients with stroke from acute anterior circulation proximal arterial occlusion, thrombectomy improves performance on the TMT at 3 months.
© 2016 American Academy of Neurology.
Figures
References
-
- Patel MD, Coshall C, Rudd AG, Wolfe CD. Cognitive impairment after stroke: clinical determinants and its associations with long-term stroke outcomes. J Am Geriatr Soc 2002;50:700–706. - PubMed
-
- Jokinen H, Melkas S, Ylikoski R, et al. . Post-stroke cognitive impairment is common even after successful clinical recovery. Eur J Neurol 2015;22:1288–1294. - PubMed
-
- Nys GM, van Zandvoort MJ, de Kort PL, et al. . The prognostic value of domain-specific cognitive abilities in acute first-ever stroke. Neurology 2005;64:821–827. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials