

Glucocorticoid-associated worsening in reversible cerebral vasoconstriction syndrome
- PMID: 27940651
- PMCID: PMC5272793
- DOI: 10.1212/WNL.0000000000003510
Glucocorticoid-associated worsening in reversible cerebral vasoconstriction syndrome
Abstract
Objective: Factors predicting poor outcome in patients with the reversible cerebral vasoconstriction syndrome (RCVS) have not been identified.
Methods: In this single-center retrospective study, we analyzed the clinical, brain imaging, and angiography data in 162 patients with RCVS. Univariable and multivariable regression analysis were performed to identify predictors of persistent (nontransient) clinical worsening, radiologic worsening, early angiographic progression, and poor discharge outcome (modified Rankin Scale score 4-6).
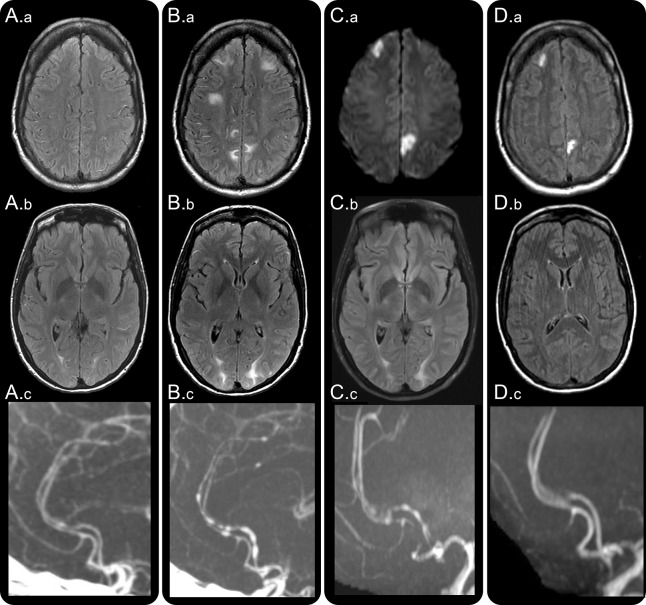
Results: The mean age was 44 ± 13 years; 78% of patients were women. Persistent clinical worsening occurred in 14% at 6.6 ± 4.1 days after symptom onset, radiologic worsening in 27% (mainly new infarcts), and angiographic progression in 15%. Clinical worsening correlated with angiographic progression and new nonhemorrhagic lesions. Age and sex did not independently predict any type of worsening. Infarction on baseline imaging predicted poor outcome. Prior serotonergic antidepressant use predicted clinical and angiographic worsening but not poor outcome. Intra-arterial vasodilator therapy independently predicted clinical worsening and poor discharge outcome but was offered to more severe cases. Glucocorticoid treatment proved to be an independent predictor of clinical, imaging, and angiographic worsening and poor outcome. Of the 23 patients with clinical worsening, 17 received glucocorticoids (15 within the preceding 2 days). There were no significant differences in baseline brain lesions and angiographic abnormalities between glucocorticoid-treated and untreated patients.
Conclusion: Patients with RCVS at risk for worsening can be identified on basis of baseline features. Iatrogenic factors such as glucocorticoid exposure may contribute to worsening.
© 2016 American Academy of Neurology.
Figures

Comment in
-
Avoidance of steroids in the reversible cerebral vasoconstriction syndrome.Neurology. 2017 Jan 17;88(3):224-225. doi: 10.1212/WNL.0000000000003521. Epub 2016 Dec 9. Neurology. 2017. PMID: 27940649 No abstract available.
References
-
- Calabrese LH, Dodick DW, Schwedt TJ, Singhal AB. Narrative review: reversible cerebral vasoconstriction syndromes. Ann Intern Med 2007;146:34–44. - PubMed
-
- Ducros A, Boukobza M, Porcher R, Sarov M, Valade D, Bousser MG. The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome: a prospective series of 67 patients. Brain 2007;130:3091–3101. - PubMed
-
- Chen SP, Fuh JL, Wang SJ, et al. . Magnetic resonance angiography in reversible cerebral vasoconstriction syndromes. Ann Neurol 2010;67:648–656. - PubMed
-
- Ducros A, Fiedler U, Porcher R, Boukobza M, Stapf C, Bousser MG. Hemorrhagic manifestations of reversible cerebral vasoconstriction syndrome: frequency, features, and risk factors. Stroke 2010;41:2505–2511. - PubMed
-
- Topcuoglu MA, Singhal AB. Hemorrhagic reversible cerebral vasoconstriction syndrome: features and mechanisms. Stroke 2016;47:1742–1747. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical