Erythrodermic Psoriasis Treated with Apremilast
- PMID: 27942369
- PMCID: PMC5134687
- DOI: 10.4081/dr.2016.6599
Erythrodermic Psoriasis Treated with Apremilast
Abstract
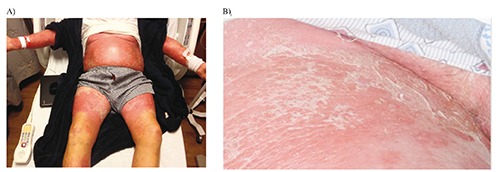
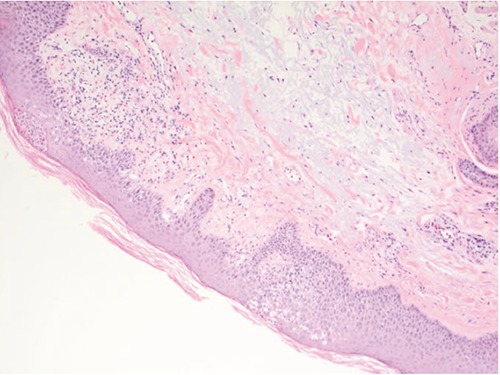
Erythroderma is a rare potentially deadly exfoliative dermatitis characterized by diffuse cutaneous erythema which may be associated with multi-organ dysfunction. Therefore, it is imperative to recognize and treat it promptly. Erythrodermic psoriasis is the most common form of erythroderma. Management of this condition is largely based on aggressive supportive care and the use of anti-inflammatory immunosuppressive and biologic agents. We describe a case of psoriatic erythroderma which was triggered by withdrawal from systemic steroids and successfully treated with apremilast and cyclosporine. Apremilast induced atrial fibrillation limited its continued use after the initial response period.
Keywords: Apremilast; Erythroderma; Erythrodermic psoriasis; Psoriasis.
Conflict of interest statement
the authors declare no potential conflict of interest.
Figures

References
-
- Rothe MJ, Bernstein ML, Grant-Kels JM. Life-threatening erythroderma: diagnosing and treating the red man. Clin Dermatol 2005;23:206-17. - PubMed
-
- Stinco G, Errichetti E. Erythrodermic psoriasis: current and future role of biologicals. Bio Drugs 2015;29:91-101. - PubMed
-
- Raychaudhuri SK, Maverakis E, Raychaudhuri SP. Diagnosis and classification of psoriasis. Autoimmun Rev 2014;13:490-5. - PubMed
-
- Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: sections 1,3,4,5. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol 2008;58:826-50. - PubMed
-
- Rosenbach M, Hsu S, Korman NJ, et al. Treatment of erythrodermic psoriasis: from the medical board of the National Psoriasis Foundation. J Am Acad Dermatol 2010;62:655-62. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources