

Robotic mitral valve surgery: overview, methodology, results, and perspective
- PMID: 27942486
- PMCID: PMC5135549
- DOI: 10.21037/acs.2016.03.16
Robotic mitral valve surgery: overview, methodology, results, and perspective
Abstract
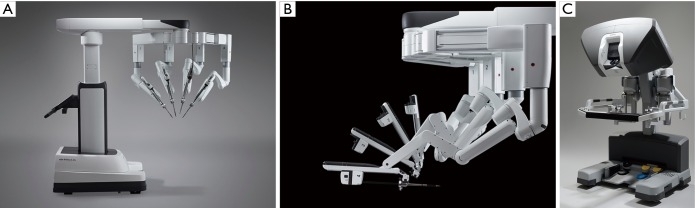
Robotic mitral valve repair began in 1998 and has advanced remarkably. It arose from an interest in reducing patient trauma by operating through smaller incisions with videoscopic assistance. In the United States, following two clinical trials, the FDA approved the daVinci Surgical System in 2002 for intra-cardiac surgery. This device has undergone three iterations, eventuating in the current daVinci XI. At present it is the only robotic device approved for mitral valve surgery. Many larger centers have adopted its use as part of their routine mitral valve repair armamentarium. Although these operations have longer perfusion and arrest times, complications have been either similar or less than other traditional methods. Preoperative screening is paramount and leads to optimal patient selection and outcomes. There are clear contraindications, both relative and absolute, that must be considered. Three-dimensional (3D) echocardiographic studies optimally guide surgeons in operative planning. Herein, we describe the selection criteria as well as our operative management during a robotic mitral valve repair. Major complications are detailed with tips to avoid their occurrence. Operative outcomes from the author's series as well as those from the largest experiences in the United States are described. They show that robotic mitral valve repair is safe and effective, as well as economically reasonable due to lower costs of hospitalization. Thus, the future of this operative technique is bright for centers adopting the "heart team" approach, adequate clinical volume and a dedicated and experienced mitral repair surgeon.
Keywords: Robot; daVinci system; mitral valve; repair; robot-assisted.
Conflict of interest statement
The author has no conflicts of interest to declare.
Figures

References
-
- Fann JI, Pompili MF, Burdon TA, et al. Minimally invasive mitral valve surgery. Semin Thorac Cardiovasc Surg 1997;9:320-30. - PubMed
-
- Dávila JC. The birth of intracardiac surgery: a semicentennial tribute (June 10, 1948-1998). Ann Thorac Surg 1998;65:1809-20. - PubMed
-
- Harken DE, Glidden EM. Experiments in Intracardiac Surgery. II. Intracardiac Visualization. J Thorac Surg 1943;12:566-72.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources