

Risk of Herpes Zoster in Individuals on Biologics, Disease-Modifying Antirheumatic Drugs, and/or Corticosteroids for Autoimmune Diseases: A Systematic Review and Meta-Analysis
- PMID: 27942537
- PMCID: PMC5144657
- DOI: 10.1093/ofid/ofw205
Risk of Herpes Zoster in Individuals on Biologics, Disease-Modifying Antirheumatic Drugs, and/or Corticosteroids for Autoimmune Diseases: A Systematic Review and Meta-Analysis
Abstract
Background: Studies examining the risk of herpes zoster (HZ) associated with immunosuppressants, such as biologics, nonbiological disease-modifying antirheumatic drugs (nbDMARDs), or corticosteroids, have generated conflicting results.
Methods: We conducted a systematic literature search from January 1946 to February 2016. Search terms related to HZ, rheumatoid arthritis, psoriasis, psoriatic arthritis, systemic lupus erythematous, or inflammatory bowel disease, biologics, nbDMARDS, and corticosteroids were used. We included randomized controlled trials (RCTs) and observational studies reporting associations between immunosuppressants and HZ outcomes in adults. For RCTs, we used the Mantel-Haenszel fixed-effects model to estimate pooled odds ratios (ORs) and 95% confidence intervals (CIs) for HZ risk. For observational studies, adjusted ORs were pooled separately using random-effects inverse variance models.
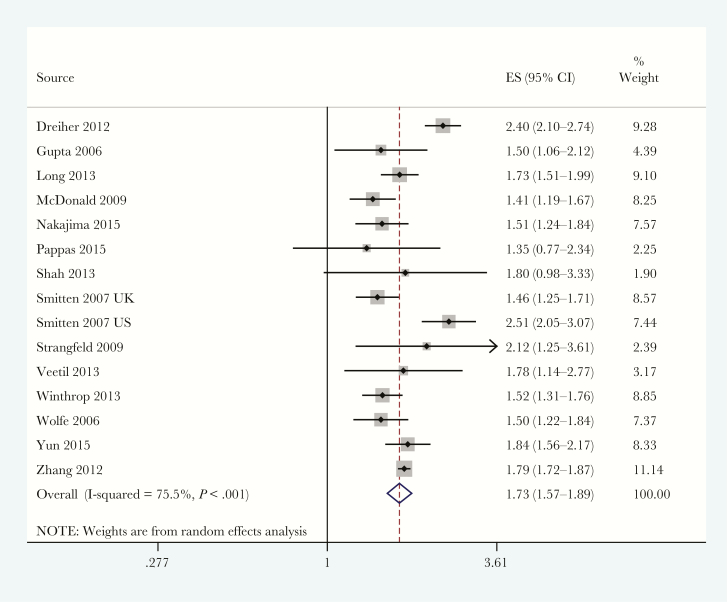
Results: Data were pooled from 40 eligible RCTs (20136 patients) and 19 observational studies (810939 patients). Biologics were associated with a greater risk of HZ than control (RCTs: OR = 1.71, 95% CI = 1.11-2.64; observational studies: OR = 1.58, 95% CI = 1.39-1.81). In RCTs, the OR of non-tumor necrosis factor (TNF) blockers was 2.19 (95% CI 1.20-4.02), but that of TNF blockers was not significantly different from control. Increased risks of HZ with nbDMARDs (OR = 1.21; 95% CI = 1.15-1.28) and corticosteroids (OR = 1.73; 95% CI = 1.57-1.89) were observed in observational studies, but few RCTs examined these comparisons.
Conclusions: Immunocompromised patients receiving biologics were associated with an increased risk of HZ. The risk is also increased with corticosteroids and nbDMARDs. These findings raise the issue of prophylaxis with zoster vaccine in patients initiating immunosuppressive therapy for autoimmune diseases.
Keywords: DMARDs; biologics; herpes zoster; immunocompromised; rheumatoid arthritis..
© The Author 2016. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Figures





References
-
- Kost RG, Straus SE. Postherpetic neuralgia–pathogenesis, treatment, and prevention. N Engl J Med 1996; 335:32–42. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
