

NT-proBNP during and after primary PCI for improved scheduling of early hospital discharge
- PMID: 27943177
- PMCID: PMC5355383
- DOI: 10.1007/s12471-016-0935-2
NT-proBNP during and after primary PCI for improved scheduling of early hospital discharge
Abstract
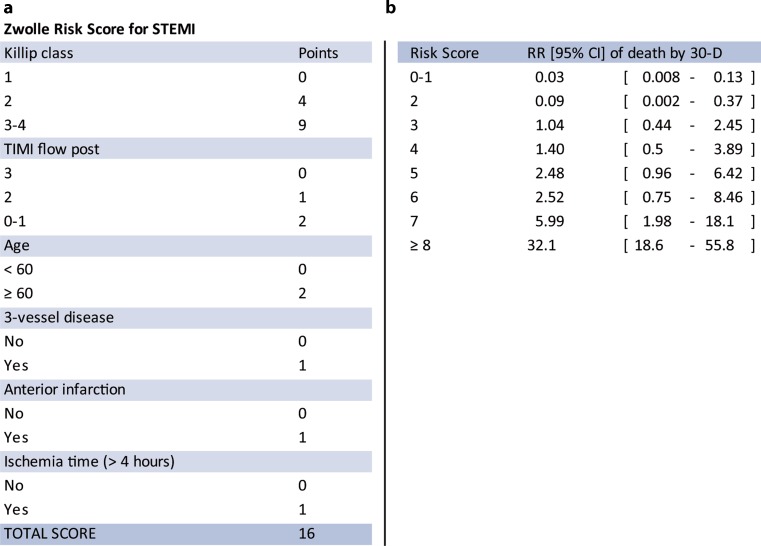
Background: The Zwolle Risk Score (ZRS) identifies primary percutaneous coronary intervention (PPCI) patients at low mortality risk, eligible for early discharge. Recently, this score was improved by adding baseline NT-proBNP. However, the optimal timepoint for NT-proBNP measurement is unknown.
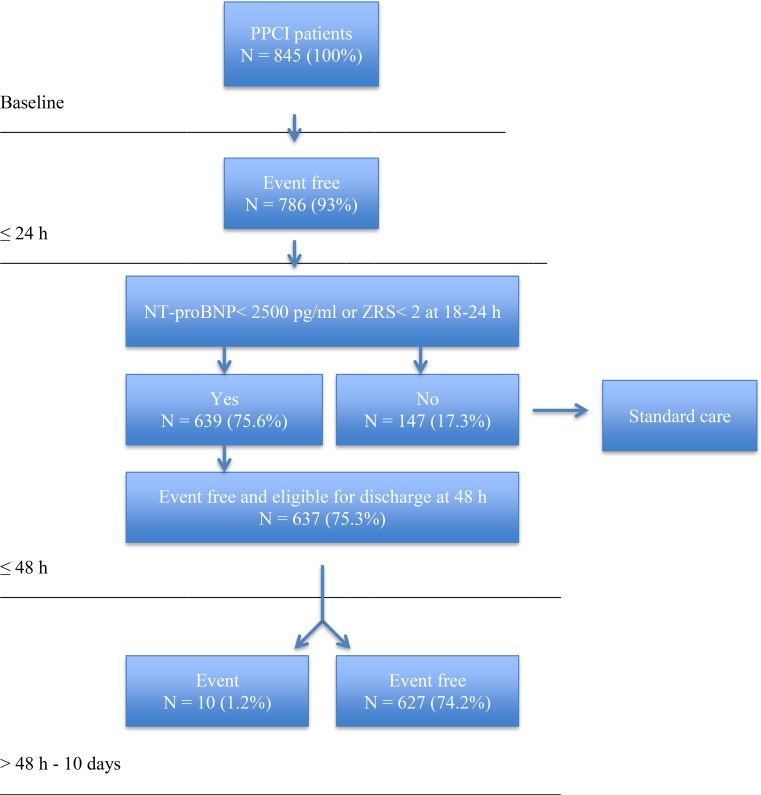
Methods: PPCI patients in the On-Time 2 study were candidates. The ZRS and NT-proBNP levels on admission, at 18-24 h, at 72-96 h, and the change in NT-proBNP from baseline to 18-24 h (delta NT-proBNP) were determined. We investigated whether addition of the different NT-proBNP measurements to the ZRS improves the prediction of 30-day mortality. Based on cut-off values reflecting zero mortality at 30 d, patients who potentially could be discharged early were identified and occurrence of major adverse cardiac events (MACE) and major bleeding until 10 d was registered.
Results: 845 patients were included. On multivariate analyses, NT-proBNP at baseline (HR 2.09, 95% CI 1.59-2.74, p < 0.001), at 18-24 h (HR 6.83, 95% CI 2.94-15.84), and at 72-96 h (HR 3.32, 95% CI 1.22-9.06) independently predicted death at 30 d. Addition of NT-proBNP to the ZRS improved prediction of mortality, particularly at 18-24 h (net reclassification index 29%, p < 0.0001, integrated discrimination improvement 17%, p < 0.0001). Based on ZRS (<2) or NT-proBNP at 18-24 h (<2500 pg/ml) 75% of patients could be targeted for early discharge at 48 h, with expected re-admission rates of 1.2% due to MACE and/or major bleeding.
Conclusions: NT-proBNP at different timepoints improves prognostication of the ZRS. Particularly at 18-24 h post PPCI, the largest group of patients that potentially could be discharged early was identified.
Keywords: Early discharge; Major adverse cardiac events (MACE); PPCI; STEMI; Serial NT-proBNP; Zwolle Risk Score.
Conflict of interest statement
D.A.A.M. Schellings, A.W.J. van’t Hof, J.M. ten Berg, A. Elvan, E. Giannitsis, C. Hamm, H. Suryapranata and A. Adiyaman declare that they have no competing interests.
Figures
References
-
- Steg PG, James SK, Atar D, et al. The Task Force on the management of ST-segment elevation myocardial infarction of the European Society of Cardiology (ESC). ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33:2569–2619. doi: 10.1093/eurheartj/ehs289. - DOI - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, et al. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA Guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362–e425. doi: 10.1161/CIR.0b013e3182742cf6. - DOI - PubMed
-
- Grines CL, Marsalese DL, Brodie B, et al. Safety and cost-effectiveness of early discharge after primary angioplasty in low risk patients with acute myocardial infarction. PAMI-II investigators. Primary angioplasty in myocardial infarction. J Am Coll Cardiol. 1998;5:967–972. doi: 10.1016/S0735-1097(98)00031-X. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
