

Differences in Managing Anticoagulants and Antiplatelets for Gastrointestinal Endoscopy between East and West
- PMID: 27956957
- PMCID: PMC5139821
- DOI: 10.4021/gr2009.04.1283
Differences in Managing Anticoagulants and Antiplatelets for Gastrointestinal Endoscopy between East and West
Abstract
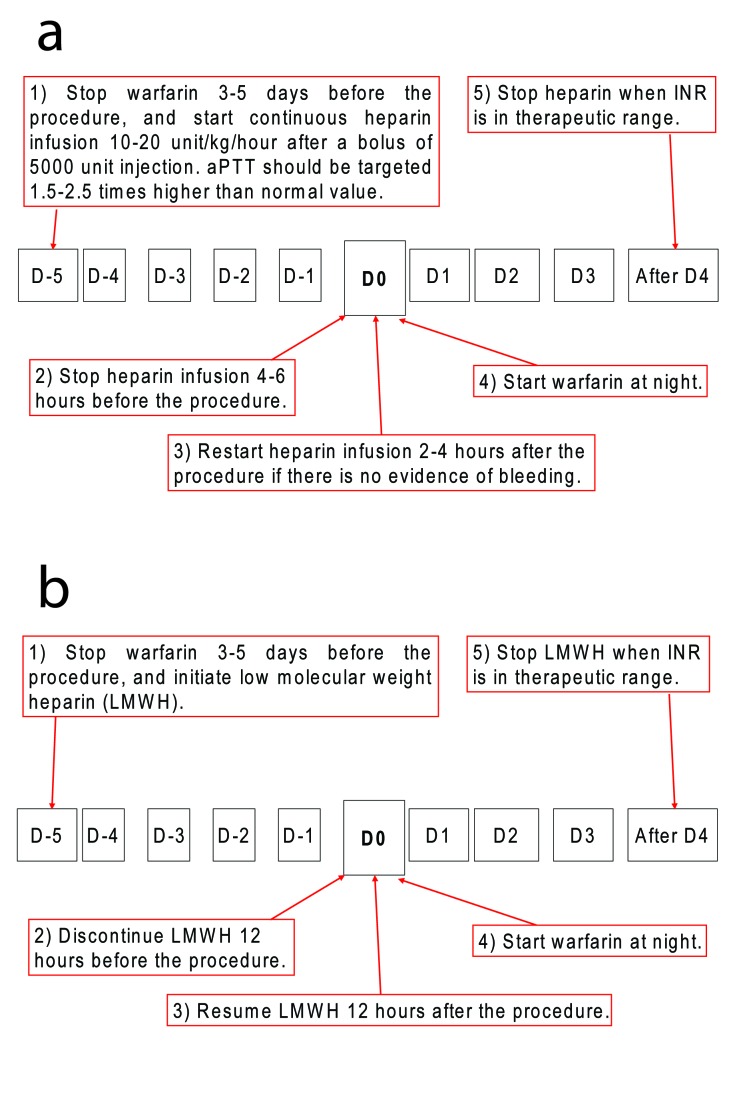
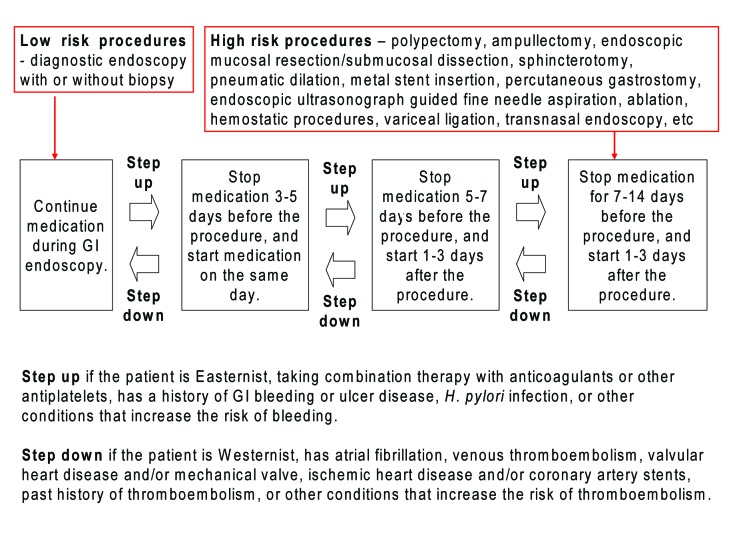
Decreasing the bleeding risk associated with gastrointestinal (GI) endoscopic procedures and minimizing the thromboembolic risk of withdrawing medications are very important for the patients taking anticoagulants and antiplatelets. Western guidelines on managing anticoagulation and antiplatelet medications in GI endoscopy suggest a polypectomy with aspirin medication or a biopsy with warfarin medication. However, Eastern endoscopists' adherence to Western guidelines may be responsible for Easteners experiencing massive bleedings. During the cessation of drugs, it should be emphasized that Asians may be predisposed to different forms of embolism more likely to be of the cerebrovascular system, whereas Westerners more likely to be of the cardiovascular variety. To better understand the differences between the East and West, differences in drug metabolism should be considered that results in greater body weight-normalized plasma unbound clearance of drug in Easterners. Taken as a whole, different managements are required for GI endoscopy in patients on anticoagulation and/or antiplatelet medications based on differences in metabolism of drugs, risk of hemorrhage, and forms of thromboembolism.
Keywords: Anticoagulation; Antiplatelet; East; Endoscopy; West.
Figures
Similar articles
-
Managing anticoagulation and antiplatelet medications in GI endoscopy: a survey comparing the East and the West.Gastrointest Endosc. 2008 Jun;67(7):1076-81. doi: 10.1016/j.gie.2007.11.037. Epub 2008 Apr 2. Gastrointest Endosc. 2008. PMID: 18384789
-
[Anticoagulation and antiplatelet therapy, and gastrointestinal endoscopy].Orv Hetil. 2009 Mar 22;150(12):541-8. doi: 10.1556/OH.2009.28554. Orv Hetil. 2009. PMID: 19275971 Review. Hungarian.
-
Anticoagulation and antiplatelet management in gastrointestinal endoscopy: A review of current evidence.World J Gastrointest Endosc. 2020 Nov 16;12(11):408-450. doi: 10.4253/wjge.v12.i11.408. World J Gastrointest Endosc. 2020. PMID: 33269053 Free PMC article. Review.
-
Therapeutic endoscopy-related GI bleeding and thromboembolic events in patients using warfarin or direct oral anticoagulants: results from a large nationwide database analysis.Gut. 2018 Oct;67(10):1805-1812. doi: 10.1136/gutjnl-2017-313999. Epub 2017 Sep 5. Gut. 2018. PMID: 28874418 Free PMC article.
-
Antiplatelet and anticoagulant drugs management before gastrointestinal endoscopy: do clinicians adhere to current guidelines?Dig Liver Dis. 2015 Jan;47(1):45-9. doi: 10.1016/j.dld.2014.10.017. Epub 2014 Nov 1. Dig Liver Dis. 2015. PMID: 25464898
Cited by
-
A guideline to fill the gap between endoscopists and physicians who prescribe anticoagulant and/or antiplatelet agents.J Gastroenterol. 2010 May;45(5):568-9; author reply 570. doi: 10.1007/s00535-010-0225-5. Epub 2010 Mar 9. J Gastroenterol. 2010. PMID: 20213335 No abstract available.
-
Current progress toward eradicating Helicobacter pylori in East Asian countries: differences in the 2013 revised guidelines between China, Japan, and South Korea.World J Gastroenterol. 2014 Feb 14;20(6):1493-502. doi: 10.3748/wjg.v20.i6.1493. World J Gastroenterol. 2014. PMID: 24587624 Free PMC article. Review.
-
Real-World Bleeding Risk of Anticoagulant and Nonsteroidal Anti-inflammatory Drugs Combotherapy versus Anticoagulant Monotherapy.Gut Liver. 2024 Sep 15;18(5):824-833. doi: 10.5009/gnl230541. Epub 2024 May 10. Gut Liver. 2024. PMID: 38726558 Free PMC article.
References
-
- Zuckerman MJ, Hirota WK, Adler DG, Davila RE, Jacobson BC, Leighton JA, Qureshi WA. et al. ASGE guideline: the management of low-molecular-weight heparin and nonaspirin antiplatelet agents for endoscopic procedures. Gastrointest Endosc. 2005;61:189–194. doi: 10.1016/S0016-5107(04)02392-2. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources