

Predicting Acute Pancreatitis Severity: Comparison of Prognostic Scores
- PMID: 27957018
- PMCID: PMC5139846
- DOI: 10.4021/gr364w
Predicting Acute Pancreatitis Severity: Comparison of Prognostic Scores
Abstract
Background: Acute pancreatitis has a broad clinical spectrum, from mild illness to multiple organ failure and death. Prognostic scores have been developed or adapted to predict disease severity. This study aimed to compare the prognostic scores according to sensitivity and specificity, receiver operating characteristic curves and area under the curve. Statistical correlation with disease severity, length of hospital stay, mortality and complication rates.
Methods: Retrospective analysis of the clinical data of patients admitted to an Internal Medicine ward with the diagnosis of acute pancreatitis over a ten year period. Evaluation of prognostic scores: Ranson, Glasgow-Imrie, Balthazar, APACHE II (admission and at 48 hours) and C-reactive protein (48 hours), was carried out as well as statistical analysis using Microsoft Excel 2007® and SPSS 16®. The confidence interval used was 95%.
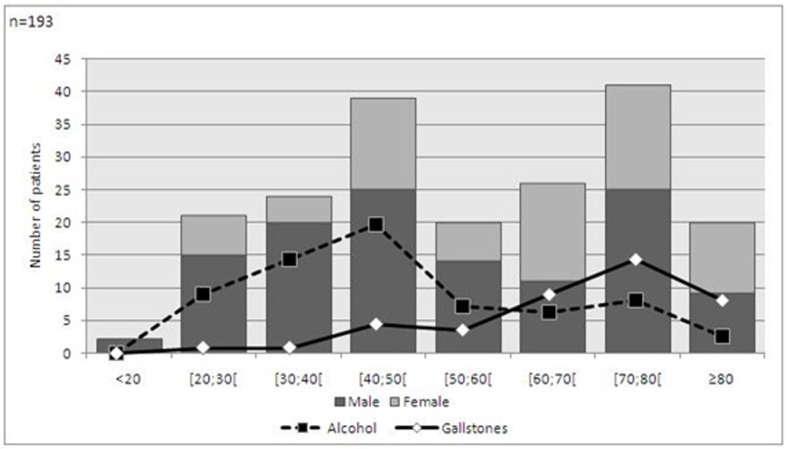
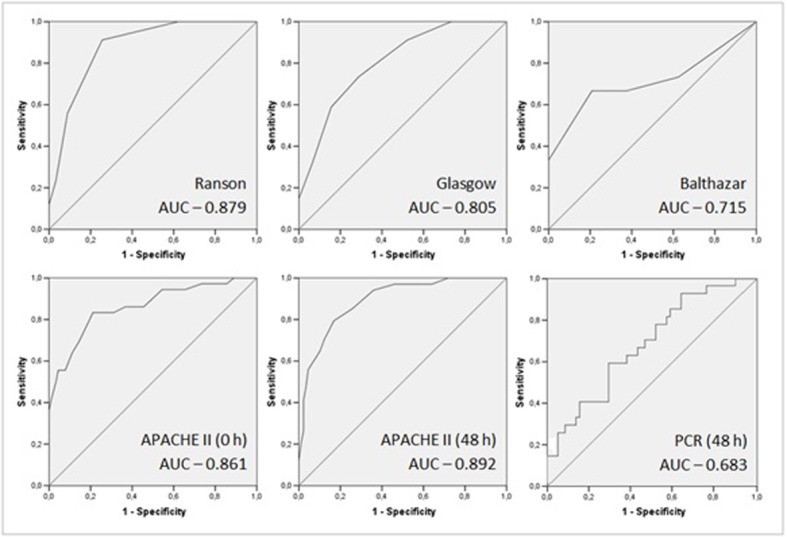
Results: Data from 193 clinical files was collected. However, 67 were excluded due to lack of information. According to the Atlanta criteria, 90 cases were deemed as mild and 36 severe. The mortality rate was 6% and the local complication rate was 9.3%. Ranson, Glasgow and APACHE II scores had significant correlation with mortality. Apart from C-reactive protein levels at 48 hours, all scores had significant correlation with disease severity. The scores with best area under the curve correlation were APACHE II (48 hours): 0.892, Ranson: 0.879, and APACHE II (admission): 0.861.
Conclusions: The most accurate prognostic scores in this study were APACHE II (48 hours) and Ranson. APACHE II at admission was a good indicator, impaired only by high false positive ratio.
Keywords: APACHE II; Acute Pancreatitis; Balthazar; C-reactive Protein; Glasgow; Prognostic Scores; Ranson.
Figures
References
-
- Bradley EL 3rd. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg. 1993;128(5):586–590. - PubMed
-
- Ranson JH, Rifkind KM, Roses DF, Fink SD, Eng K, Spencer FC. Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet. 1974;139(1):69–81. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials