

Risks Related To Fluoroscopy Radiation Associated With Electrophysiology Procedures
- PMID: 27957094
- PMCID: PMC5135251
- DOI: 10.4022/jafib.1044
Risks Related To Fluoroscopy Radiation Associated With Electrophysiology Procedures
Abstract
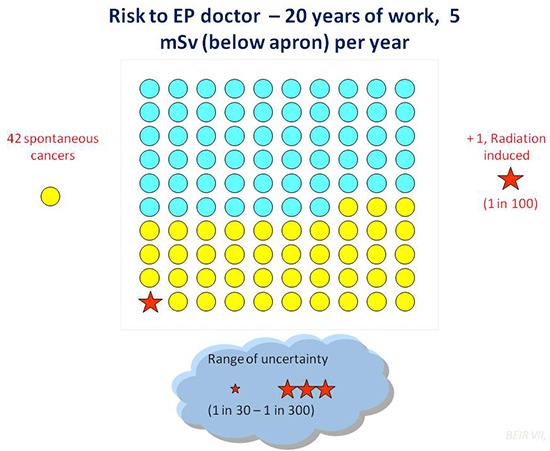
The benefits of cardiac imaging are immense, and modern cardiac electrophysiology (EP) requires the extensive and versatile use of a variety of cardiac imaging and radiology-based techniques. In the cardiac electrophysiology lab, doses can range around a reference effective dose (ED) of 15 milliSievert corresponding to 750 chest x-rays for a cardiac radiofrequency ablation, ranging from less than 2 to > 60 mSv. The reference dose for a regular pacemaker or ICD implant is 4 mSv (range 1.4-17) and for a CRT implant is 22 mSv (range 2.2-95). Doses on the order of magnitude of 10-100 milliSievert (mSv) correspond to a low (albeit definite, not negligible) additional lifetime risk of fatal and non-fatal cancer from between 1 in 1000 (10 mSv) to 1 in 100 (100 mSv). The increasing use and complexity of cardiac electrophysiology techniques have not been matched by increasing awareness and knowledge by prescribers and practitioners. The protection of doctors is just as important as protection of patients. Most experienced (and most exposed) interventional cardiologists and electrophysiologists have an exposure per annum of around 5 mSv, two to three times higher than diagnostic radiologists, with a typical cumulative lifetime attributable risk on the order of magnitude of 1 cancer (fatal and non-fatal) per 100 exposed subjects. Operator dose per procedure correlates somewhat with the patient dose, but may be typically 1000 times lower depending upon the shielding employed (one unit of incidence scatter dose for the operator when 1000 units of incident dose are given to the patient). However, adequate radiation protection training and diligent protection can reduce this radiation exposure by 90%. The priority given to radioprotection in every cardiology department is an effective strategy for primary prevention of cancer, a strong indicator of the quality of the cardiology division, and the most effective shielding for enhancing the safety of patients, doctors, and staff.
Keywords: Electrophysiology; Radiation; Risk.
Figures

References
-
- Picano Eugenio, Vañó Eliseo, Rehani Madan M, Cuocolo Alberto, Mont Lluis, Bodi Vicente, Bar Olivier, Maccia Carlo, Pierard Luc, Sicari Rosa, Plein Sven, Mahrholdt Heiko, Lancellotti Patrizio, Knuuti Juhani, Heidbuchel Hein, Di Mario Carlo, Badano Luigi P. The appropriate and justified use of medical radiation in cardiovascular imaging: a position document of the ESC Associations of Cardiovascular Imaging, Percutaneous Cardiovascular Interventions and Electrophysiology. Eur. Heart J. 2014 Mar;35 (10):665–72. - PubMed
-
- Correia Maria Joao, Hellies Arianna, Andreassi Maria Grazia, Ghelarducci Bruno, Picano Eugenio. Lack of radiological awareness among physicians working in a tertiary-care cardiological centre. Int. J. Cardiol. 2005 Sep 1;103 (3):307–11. - PubMed
-
- Kim Candice, Vasaiwala Samip, Haque Faizul, Pratap Kiran, Vidovich Mladen I. Radiation safety among cardiology fellows. Am. J. Cardiol. 2010 Jul 1;106 (1):125–8. - PubMed
-
- Picano Eugenio, Vano Eliseo. Radiation exposure as an occupational hazard. EuroIntervention. 2012 Oct;8 (6):649–53. - PubMed
-
- Heidbuchel Hein, Wittkampf Fred H M, Vano Eliseo, Ernst Sabine, Schilling Richard, Picano Eugenio, Mont Lluis, Jais Pierre, de Bono Joseph, Piorkowski Christopher, Saad Eduardo, Femenia Francisco. Practical ways to reduce radiation dose for patients and staff during device implantations and electrophysiological procedures. Europace. 2014 Jul;16 (7):946–64. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous