

Review
doi: 10.4022/jafib.1054.
eCollection 2014 Aug-Sep.
Anatomic Challenges In Pediatric Catheter Ablation
Affiliations
- PMID: 27957095
- PMCID: PMC5135252
- DOI: 10.4022/jafib.1054
Item in Clipboard
Review
Anatomic Challenges In Pediatric Catheter Ablation
J Atr Fibrillation.
.
Abstract
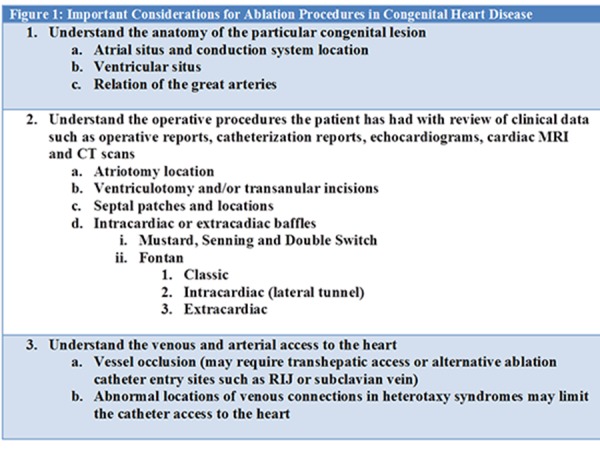
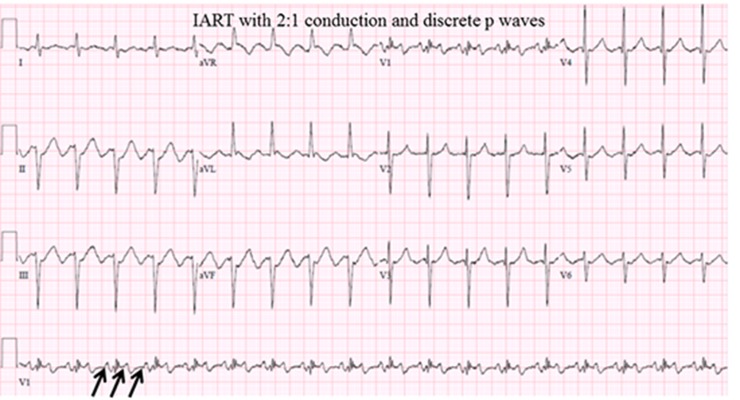
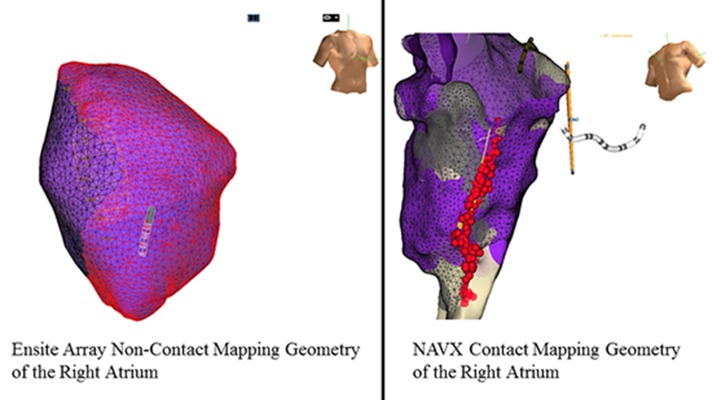
Pediatric patients present unique anatomic challenges for catheter ablation. Small patient size requires special adaptation and understanding to perform safe procedures when clinically indicated. The anatomic variations of congenital heart disease also create problems that require pre-procedural preparation for each case in addition to a specialized understanding of a vast anatomic variation and surgical repairs. This understanding coupled with the knowledge of the pathophysiology of arrhythmia disorders and the biophysics of catheter ablation technology are required to perform successful and safe ablation procedures in this special population.
Figures


References
-
- Van Hare G F, Velvis H, Langberg J J. Successful transcatheter ablation of congenital junctional ectopic tachycardia in a ten-month-old infant using radiofrequency energy. Pacing Clin Electrophysiol. 1990 Jun;13 (6):730–5. - PubMed
-
- Tanel R E, Walsh E P, Triedman J K, Epstein M R, Bergau D M, Saul J P. Five-year experience with radiofrequency catheter ablation: implications for management of arrhythmias in pediatric and young adult patients. J. Pediatr. 1997 Dec;131 (6):878–87. - PubMed
-
- Kugler J D, Danford D A, Deal B J, Gillette P C, Perry J C, Silka M J, Van Hare G F, Walsh E P. Radiofrequency catheter ablation for tachyarrhythmias in children and adolescents. The Pediatric Electrophysiology Society. N. Engl. J. Med. 1994 May 26;330 (21):1481–7. - PubMed
-
- Kugler J D, Danford D A, Houston K, Felix G. Radiofrequency catheter ablation for paroxysmal supraventricular tachycardia in children and adolescents without structural heart disease. Pediatric EP Society, Radiofrequency Catheter Ablation Registry. Am. J. Cardiol. 1997 Dec 1;80 (11):1438–43. - PubMed
-
- Friedman Richard A, Walsh Edward P, Silka Michael J, Calkins Hugh, Stevenson William G, Rhodes Larry A, Deal Barbara J, Wolff Grace S, Demaso David R, Hanisch Debra, Van Hare George F. NASPE Expert Consensus Conference: Radiofrequency catheter ablation in children with and without congenital heart disease. Report of the writing committee. North American Society of Pacing and Electrophysiology. Pacing Clin Electrophysiol. 2002 Jun;25 (6):1000–17. - PubMed
Publication types
LinkOut - more resources
Full Text Sources