

Idiopathic Ventricular Tachycardia: Transcatheter Ablation or Antiarrhythmic Drugs?
- PMID: 27957145
- PMCID: PMC5135213
- DOI: 10.4022/jafib.1164
Idiopathic Ventricular Tachycardia: Transcatheter Ablation or Antiarrhythmic Drugs?
Abstract
Introduction: Ventricular tachycardia or frequent premature ventricular contractions (PVCs) can occur in the absence of any detectable structural heart disease. In this clinical setting, these arrhythmias are termed idiopathic. Usually, they carry a benign prognosis and any potential ablative intervention is carried out if patients are highly symptomatic or, more importantly, if frequent ventricular arrhythmias can lead to ventricular dysfunction.
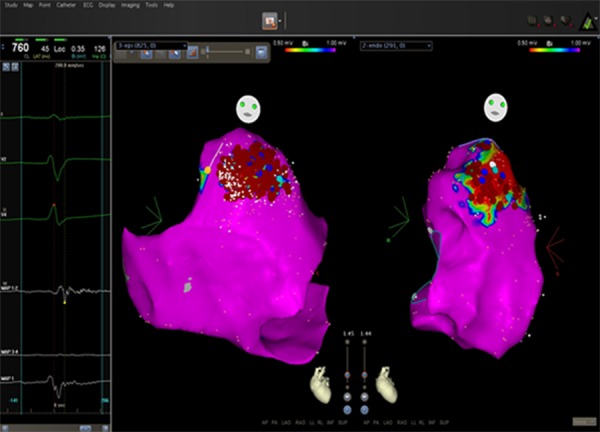
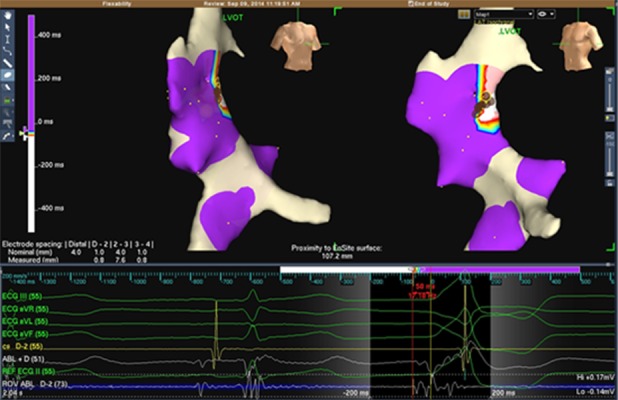
Methods: In this paper, different forms of idiopathic ventricular tachycardia are reviewed. Outflow tract ventricular tachycardia from the right ventricle is the most frequent form of the so-called idiopathic ventricular tachycardia. Other forms of idiopathic ventricular arrhythmias include ventricular tachycardia/PVCs arising from tricuspid annulus, from the mitral annulus, inter-fascicular ventricular tachycardia and papillary muscle ventricular tachycardia. When interventional treatment is deemed necessary, detailed mapping ( earliest activation during VT/PVC, pace mapping ) is crucial as to identify the successful ablation site. Catheter ablation more than antiarrhythmic drug treatment is usually highly effective in eliminating idiopathic ventricular arrhythmias and providing prevention of recurrence.
Conclusions: Idiopathic VTs are not considered life-threatening arrhythmias and, prevention of recurrences is often achieved by means of catheter ablation that provides an improvement of quality of life. The overall acute success rate of catheter ablation is about 85-90% with a long-term prevention of arrhythmia recurrence of about 75-80%. It is advisable that the procedure is carried out by electrophysiologists with expertise in VT catheter ablation and extensive knowledge of cardiac anatomy as to ensure a high success rate and reduce the likelihood of major complications.
Figures
References
-
- Aliot Etienne M, Stevenson William G, Almendral-Garrote Jesus Ma, Bogun Frank, Calkins C Hugh, Delacretaz Etienne, Della Bella Paolo, Hindricks Gerhard, Jaïs Pierre, Josephson Mark E, Kautzner Josef, Kay G Neal, Kuck Karl-Heinz, Lerman Bruce B, Marchlinski Francis, Reddy Vivek, Schalij Martin-Jan, Schilling Richard, Soejima Kyoko, Wilber David. EHRA/HRS Expert Consensus on Catheter Ablation of Ventricular Arrhythmias: developed in a partnership with the European Heart Rhythm Association (EHRA), a Registered Branch of the European Society of Cardiology (ESC), and the Heart Rhythm Society (HRS); in collaboration with the American College of Cardiology (ACC) and the American Heart Association (AHA). Heart Rhythm. 2009 Jun;6 (6):886–933. - PubMed
-
- Azegami Koji, Wilber David J, Arruda Mauricio, Lin Albert C, Denman Russell A. Spatial resolution of pacemapping and activation mapping in patients with idiopathic right ventricular outflow tract tachycardia. J. Cardiovasc. Electrophysiol. 2005 Aug;16 (8):823–9. - PubMed
-
- Daniels David V, Lu Yen-Yu, Morton Joseph B, Santucci Peter A, Akar Joseph G, Green Alex, Wilber David J. Idiopathic epicardial left ventricular tachycardia originating remote from the sinus of Valsalva: electrophysiological characteristics, catheter ablation, and identification from the 12-lead electrocardiogram. Circulation. 2006 Apr 4;113 (13):1659–66. - PubMed
-
- Callans David J. Catheter ablation of idiopathic ventricular tachycardia arising from the aortic root. J. Cardiovasc. Electrophysiol. 2009 Aug;20 (8):969–72. - PubMed
-
- Hachiya Hitoshi, Aonuma Kazutaka, Yamauchi Yasuteru, Igawa Masayuki, Nogami Akihiko, Iesaka Yoshito. How to diagnose, locate, and ablate coronary cusp ventricular tachycardia. J. Cardiovasc. Electrophysiol. 2002 Jun;13 (6):551–6. - PubMed