

Social characteristics associated with disparities in smoking rates in Israel
- PMID: 27957321
- PMCID: PMC5131466
- DOI: 10.1186/s13584-016-0095-2
Social characteristics associated with disparities in smoking rates in Israel
Abstract
Background: Cigarette smoking is a major cause of health disparities. We aimed to determine social characteristics associated with smoking status and age at smoking initiation in the ethnically-diverse population of Israel.
Methods: This is a cross-sectional survey, based on data collected during 2010 by the Israel Bureau of Statistics, in a representative nationwide sample of 7,524 adults (≥20 years). Information collected by personal interviews included a broad set of demographic and socio-economic characteristics and detailed information on smoking habits. Associations between social characteristics and smoking habits were tested in multivariable regression models.
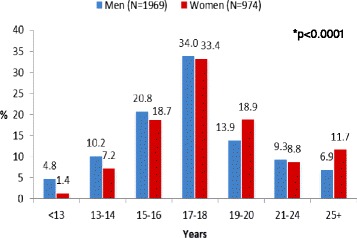
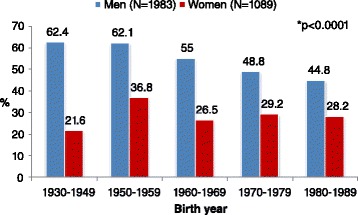
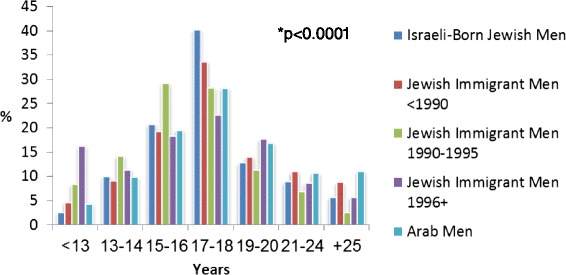
Results: Current smoking was more frequent among men than among women (30.9 % vs. 16.8 %; p < 0.0001). In multivariable regression analysis, the association of some social characteristics with smoking status differed by gender. Lower socioeconomic status (reflected by higher rate of unemployment, lower income, possession of fewer material assets, difficulty to meet living expenses) and lower educational level were significantly associated with current smoking among men but not among women. Family status other than being married was associated with higher likelihood of being a current smoker, while being traditional or observant was associated with a lower likelihood of ever smoking among both gender groups. Arab minority men and male immigrants from the former Soviet Union countries were more frequently current smokers than Israeli-born Jewish men [adjusted odds ratio (95 % confidence interval): 1.53 (1.22, 1.93) and 1.37 (1.01-1.87), respectively]. Compared to Israeli-born men, the age at smoking initiation was younger among male immigrants, and older among Arab minority men [adjusted hazard ratio (95 % confidence interval): 1.360 (1.165-1.586), and 0.849 (0.749-0.962), respectively]. While the prevalence of current smoking was lower in younger birth cohorts, the age at smoking initiation among ever-smokers declined as well.
Conclusions: Among several subgroups within the Israeli population the smoking uptake is high, e.g. Arab men, men who are less affluent, who have lower educational level, and male immigrants. These subgroups should be prioritized for intervention to reduce the burden of smoking. To be effective, gender, cultural background and socioeconomic characteristics should be considered in the design and implementation of culturally-congruent tobacco control and smoking prevention and cessation interventions.
Keywords: Cigarette smoking; Education; Ethnicity; Gender; Health disparities; Immigrant; Poverty; Smoking uptake.
Figures
Comment in
-
Racial and ethnic disparities in smoking prevalence in Israel and the United States: progress to date and prospects for the future.Isr J Health Policy Res. 2017 Oct 2;6(1):51. doi: 10.1186/s13584-017-0177-9. Isr J Health Policy Res. 2017. PMID: 28969689 Free PMC article.
References
-
- U.S. Department of Health and Human Services . The Health Consequences of Smoking: 50 Years of Progress. A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014.
-
- Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328:1519. doi: 10.1136/bmj.38142.554479.AE. - DOI - PMC - PubMed
-
- WHO. World health report 2002: reducing risks, promoting healthy life. 2002: http://www.who.int/whr/2002/en (accessed May 10, 2015). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
