

Osimertinib or Platinum-Pemetrexed in EGFR T790M-Positive Lung Cancer
- PMID: 27959700
- PMCID: PMC6762027
- DOI: 10.1056/NEJMoa1612674
Osimertinib or Platinum-Pemetrexed in EGFR T790M-Positive Lung Cancer
Abstract
Background: Osimertinib is an epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) that is selective for both EGFR-TKI sensitizing and T790M resistance mutations in patients with non-small-cell lung cancer. The efficacy of osimertinib as compared with platinum-based therapy plus pemetrexed in such patients is unknown.
Methods: In this randomized, international, open-label, phase 3 trial, we assigned 419 patients with T790M-positive advanced non-small-cell lung cancer, who had disease progression after first-line EGFR-TKI therapy, in a 2:1 ratio to receive either oral osimertinib (at a dose of 80 mg once daily) or intravenous pemetrexed (500 mg per square meter of body-surface area) plus either carboplatin (target area under the curve, 5 [AUC5]) or cisplatin (75 mg per square meter) every 3 weeks for up to six cycles; maintenance pemetrexed was allowed. In all the patients, disease had progressed during receipt of first-line EGFR-TKI therapy. The primary end point was investigator-assessed progression-free survival.
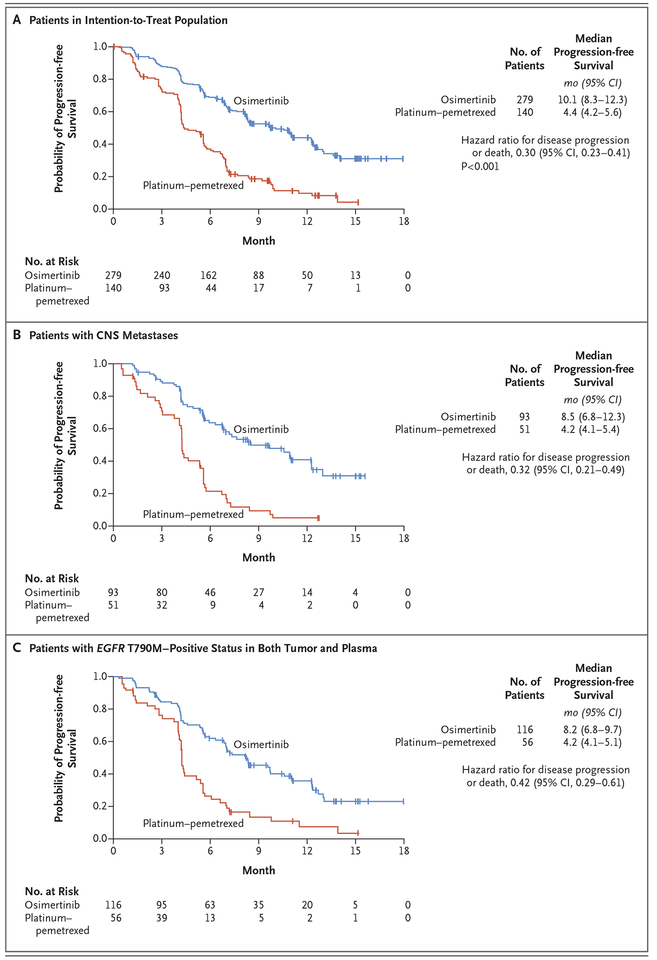
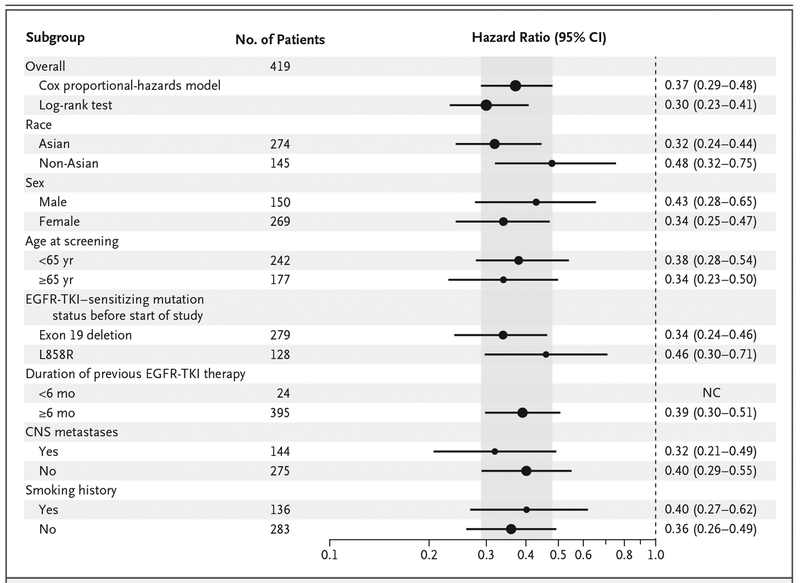
Results: The median duration of progression-free survival was significantly longer with osimertinib than with platinum therapy plus pemetrexed (10.1 months vs. 4.4 months; hazard ratio; 0.30; 95% confidence interval [CI], 0.23 to 0.41; P<0.001). The objective response rate was significantly better with osimertinib (71%; 95% CI, 65 to 76) than with platinum therapy plus pemetrexed (31%; 95% CI, 24 to 40) (odds ratio for objective response, 5.39; 95% CI, 3.47 to 8.48; P<0.001). Among 144 patients with metastases to the central nervous system (CNS), the median duration of progression-free survival was longer among patients receiving osimertinib than among those receiving platinum therapy plus pemetrexed (8.5 months vs. 4.2 months; hazard ratio, 0.32; 95% CI, 0.21 to 0.49). The proportion of patients with adverse events of grade 3 or higher was lower with osimertinib (23%) than with platinum therapy plus pemetrexed (47%).
Conclusions: Osimertinib had significantly greater efficacy than platinum therapy plus pemetrexed in patients with T790M-positive advanced non-small-cell lung cancer (including those with CNS metastases) in whom disease had progressed during first-line EGFR-TKI therapy. (Funded by AstraZeneca; AURA3 ClinicalTrials.gov number, NCT02151981 .).
Figures
Comment in
-
Lung cancer: AURA3 magic reveals new standard.Nat Rev Clin Oncol. 2017 Feb;14(2):69. doi: 10.1038/nrclinonc.2016.220. Epub 2016 Dec 29. Nat Rev Clin Oncol. 2017. PMID: 28031555 No abstract available.
-
Osimertinib improves progression-free survival in NSCLC.Lancet Respir Med. 2017 Apr;5(4):251. doi: 10.1016/S2213-2600(17)30085-1. Epub 2017 Mar 9. Lancet Respir Med. 2017. PMID: 28284589 No abstract available.
-
Osimertinib for advanced non-small cell lung cancer harboring EGFR mutation exon 20 T790M, acquired resistant mutation for first- or second-generation EGFR-TKI.J Thorac Dis. 2017 Mar;9(3):470-473. doi: 10.21037/jtd.2017.03.26. J Thorac Dis. 2017. PMID: 28449447 Free PMC article. No abstract available.
-
Osimertinib in EGFR T790M-Positive Lung Cancer.N Engl J Med. 2017 May 18;376(20):1993. doi: 10.1056/NEJMc1703339. N Engl J Med. 2017. PMID: 28514611 No abstract available.
-
Osimertinib in EGFR T790M-Positive Lung Cancer.N Engl J Med. 2017 May 18;376(20):1992-3. doi: 10.1056/NEJMc1703339. N Engl J Med. 2017. PMID: 28517914 No abstract available.
-
AURA 3: the last word on chemotherapy as a control arm in EGFR mutant NSCLC?Ann Transl Med. 2017 May;5(Suppl 1):S14. doi: 10.21037/atm.2017.03.73. Ann Transl Med. 2017. PMID: 28567396 Free PMC article. No abstract available.
References
-
- Novello S, Barlesi F, Califano R, et al. Metastatic non-small-cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2016; 27: Suppl 5: v1–v27. - PubMed
-
- Tan DS, Yom SS, Tsao MS, et al. The International Association for the Study of Lung Cancer consensus statement on optimizing management of EGFR mutation-positive non-small cell lung cancer: status in 2016. J Thorac Oncol 2016; 11: 946–63. - PubMed
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: NSCLC (version 3.2017). 2016. (http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf). - PubMed
-
- Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non–small-cell lung cancer with mutated EGFR. N Engl J Med 2010; 362: 2380–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous