

Thresholds for Abdominal Aortic Aneurysm Repair in England and the United States
- PMID: 27959727
- PMCID: PMC5177793
- DOI: 10.1056/NEJMoa1600931
Thresholds for Abdominal Aortic Aneurysm Repair in England and the United States
Abstract
Background: Thresholds for repair of abdominal aortic aneurysms vary considerably among countries.
Methods: We examined differences between England and the United States in the frequency of aneurysm repair, the mean aneurysm diameter at the time of the procedure, and rates of aneurysm rupture and aneurysm-related death. Data on the frequency of repair of intact (nonruptured) abdominal aortic aneurysms, in-hospital mortality among patients who had undergone aneurysm repair, and rates of aneurysm rupture during the period from 2005 through 2012 were extracted from the Hospital Episode Statistics database in England and the U.S. Nationwide Inpatient Sample. Data on the aneurysm diameter at the time of repair were extracted from the U.K. National Vascular Registry (2014 data) and from the U.S. National Surgical Quality Improvement Program (2013 data). Aneurysm-related mortality during the period from 2005 through 2012 was determined from data obtained from the Centers for Disease Control and Prevention and the U.K. Office of National Statistics. Data were adjusted with the use of direct standardization or conditional logistic regression for differences between England and the United States with respect to population age and sex.
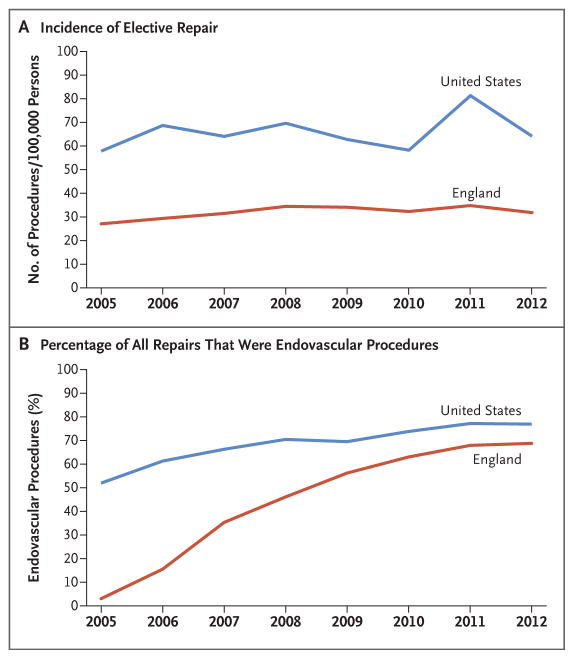
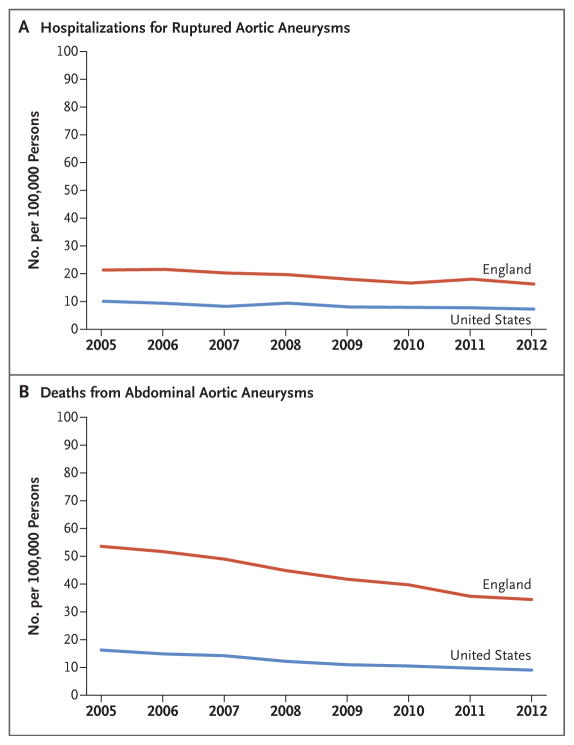
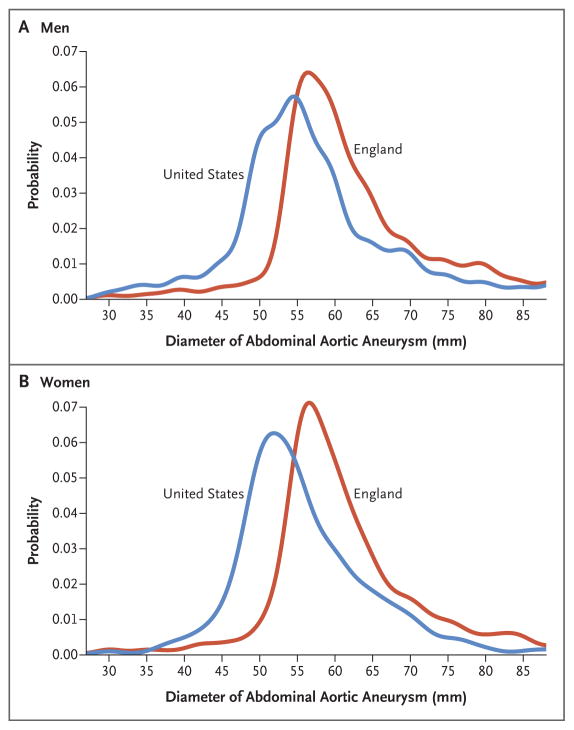
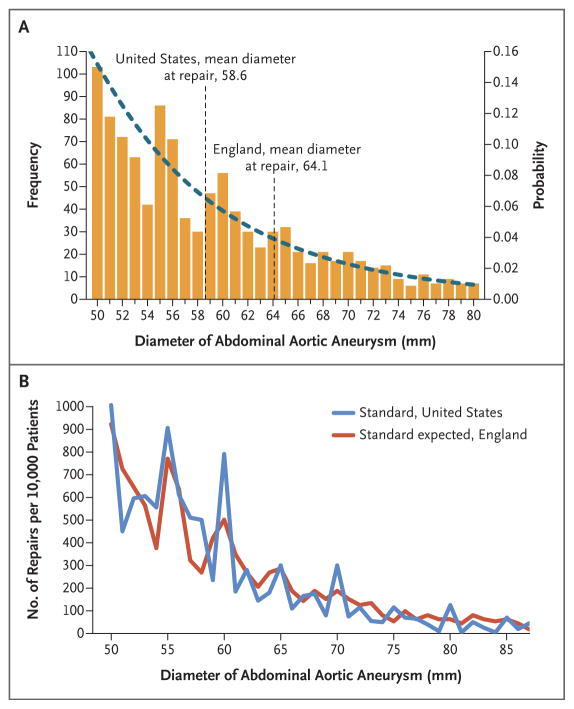
Results: During the period from 2005 through 2012, a total of 29,300 patients in England and 278,921 patients in the United States underwent repair of intact abdominal aortic aneurysms. Aneurysm repair was less common in England than in the United States (odds ratio, 0.49; 95% confidence interval [CI], 0.48 to 0.49; P<0.001), and aneurysm-related death was more common in England than in the United States (odds ratio, 3.60; 95% CI, 3.55 to 3.64; P<0.001). Hospitalization due to an aneurysm rupture occurred more frequently in England than in the United States (odds ratio, 2.23; 95% CI, 2.19 to 2.27; P<0.001), and the mean aneurysm diameter at the time of repair was larger in England (63.7 mm vs. 58.3 mm, P<0.001).
Conclusions: We found a lower rate of repair of abdominal aortic aneurysms and a larger mean aneurysm diameter at the time of repair in England than in the United States and lower rates of aneurysm rupture and aneurysm-related death in the United States than in England. (Funded by the Circulation Foundation and others.).
Conflict of interest statement
Drs. Loftus and Thompson report receiving consulting fees from Endologix, Medtronic, and Gore and grant support to their institution from Endologix and Medtronic; and Dr. Schermerhorn, receiving fees for serving on a data and safety monitoring board from Endologix and consulting fees from Endologix and Cordis. No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Abdominal Aortic Aneurysm Repair in England and the United States.N Engl J Med. 2017 Mar 9;376(10):998. doi: 10.1056/NEJMc1700463. N Engl J Med. 2017. PMID: 28273026 No abstract available.
-
Abdominal Aortic Aneurysm Repair in England and the United States.N Engl J Med. 2017 Mar 9;376(10):998. doi: 10.1056/NEJMc1700463. N Engl J Med. 2017. PMID: 28273027 No abstract available.
-
Abdominal Aortic Aneurysm Repair in England and the United States.N Engl J Med. 2017 Mar 9;376(10):997-8. doi: 10.1056/NEJMc1700463. N Engl J Med. 2017. PMID: 28276231 No abstract available.
-
Lowering Size Threshold for Elective Repair to Reduce Deaths from Abdominal Aortic Aneurysms - A Simple Solution to a Complex Problem?Eur J Vasc Endovasc Surg. 2017 Sep;54(3):275-277. doi: 10.1016/j.ejvs.2017.07.007. Epub 2017 Jul 26. Eur J Vasc Endovasc Surg. 2017. PMID: 28755854 No abstract available.
-
The World Is Not Enough: How Can "Big Data" Inform Guidelines for Elective AAA Repair?Eur J Vasc Endovasc Surg. 2020 Jun;59(6):898. doi: 10.1016/j.ejvs.2020.01.013. Epub 2020 Feb 5. Eur J Vasc Endovasc Surg. 2020. PMID: 32035743 No abstract available.
References
-
- Brady AR, Thompson SG, Fowkes FG, Greenhalgh RM, Powell JT. Abdominal aortic aneurysm expansion: risk factors and time intervals for surveillance. Circulation. 2004;110:16–21. - PubMed
-
- Lederle FA, Johnson GR, Wilson SE, et al. Rupture rate of large abdominal aortic aneurysms in patients refusing or unfit for elective repair. JAMA. 2002;287:2968–72. - PubMed
-
- Moll FL, Powell JT, Fraedrich G, et al. Management of abdominal aortic aneurysms clinical practice guidelines of the European Society for Vascular Surgery. Eur J Vasc Endovasc Surg. 2011;41(Suppl 1):S1–S58. - PubMed
-
- Mani K, Venermo M, Beiles B, et al. Regional differences in case mix and peri-operative outcome after elective abdominal aortic aneurysm repair in the Vascunet database. Eur J Vasc Endovasc Surg. 2015;49:646–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources