

Magnetic Resonance Thermometry-Guided Stereotactic Laser Ablation of Cavernous Malformations in Drug-Resistant Epilepsy: Imaging and Clinical Results
- PMID: 27959970
- PMCID: PMC4877301
- DOI: 10.1227/NEU.0000000000001033
Magnetic Resonance Thermometry-Guided Stereotactic Laser Ablation of Cavernous Malformations in Drug-Resistant Epilepsy: Imaging and Clinical Results
Abstract
Background: Surgery is indicated for cerebral cavernous malformations (CCM) that cause medically refractory epilepsy. Real-time magnetic resonance thermography (MRT)-guided stereotactic laser ablation (SLA) is a minimally invasive approach to treating focal brain lesions. SLA of CCM has not previously been described.
Objective: To describe MRT-guided SLA, a novel approach to treating CCM-related epilepsy, with respect to feasibility, safety, imaging, and seizure control in 5 consecutive patients.
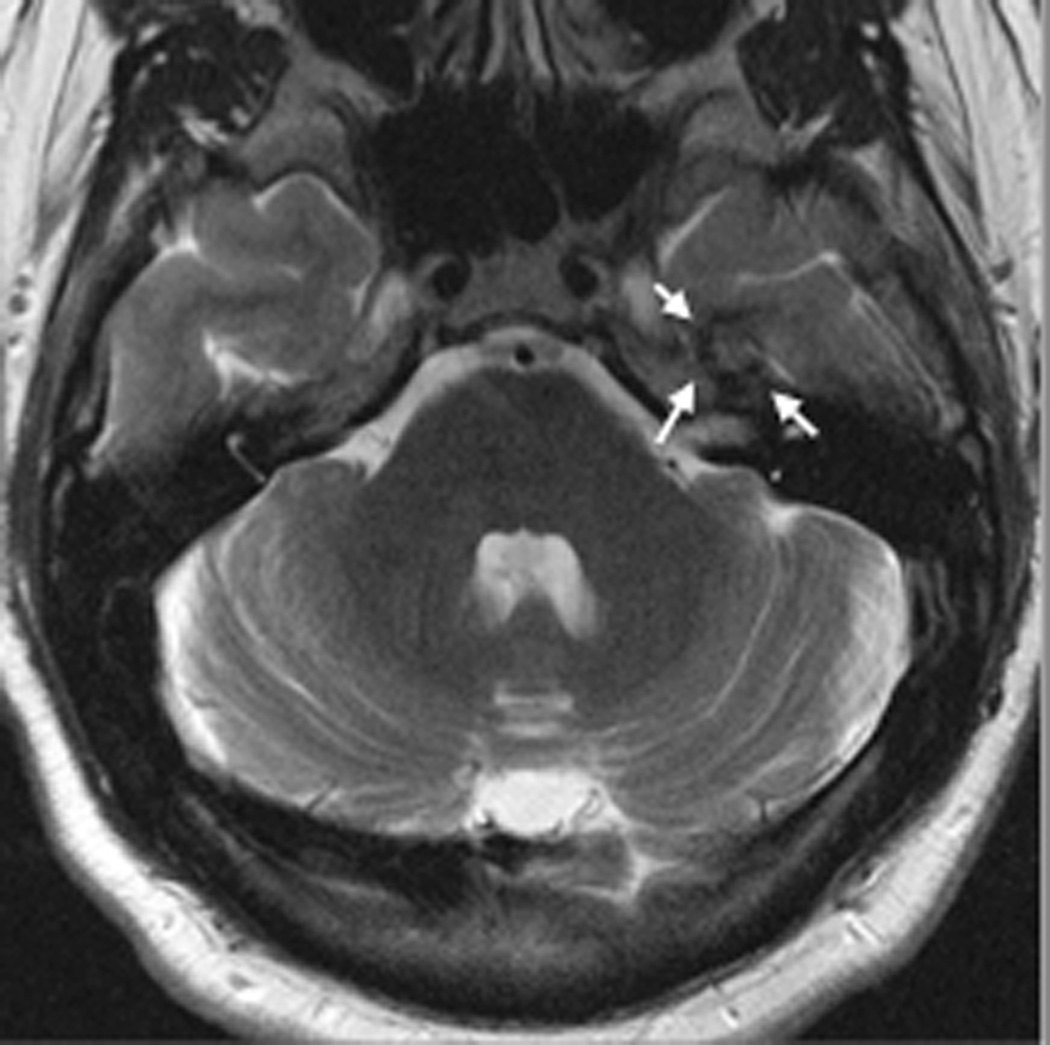
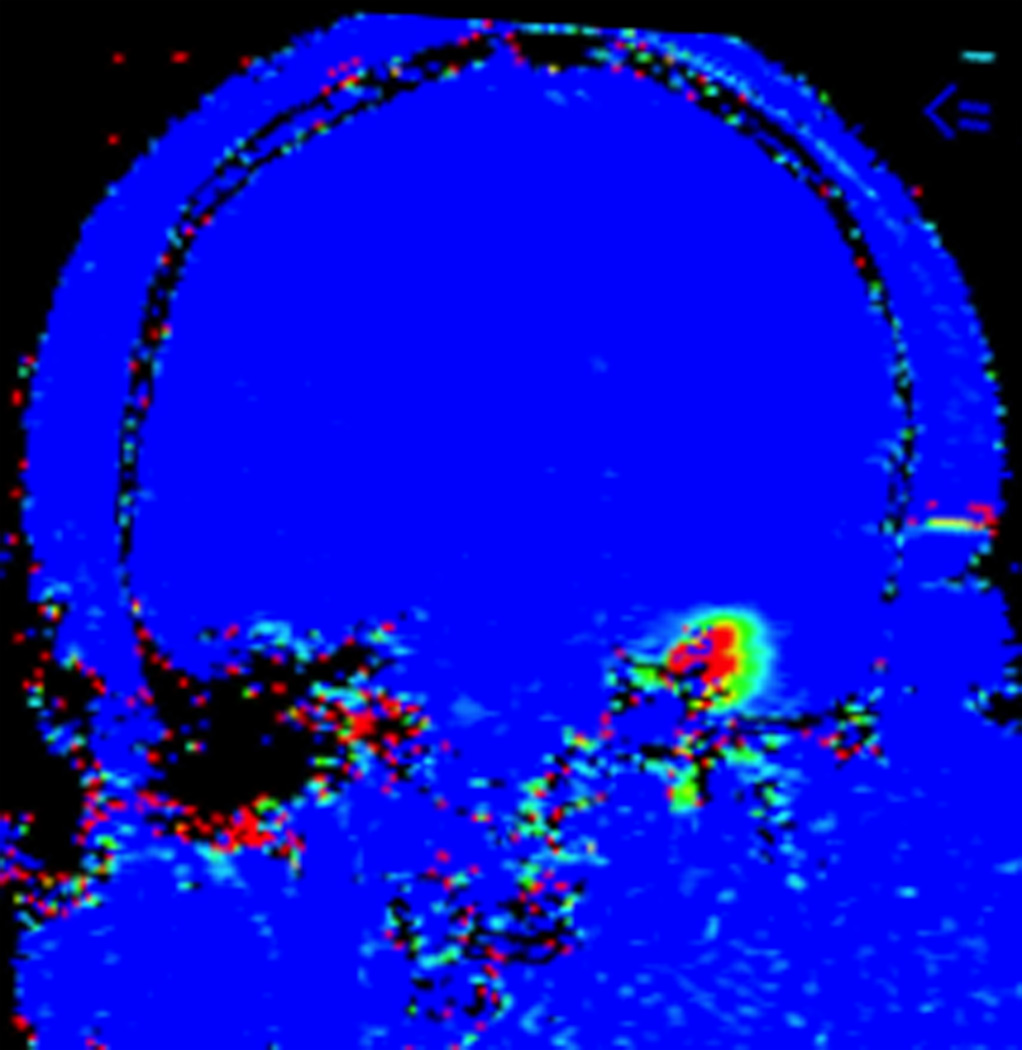
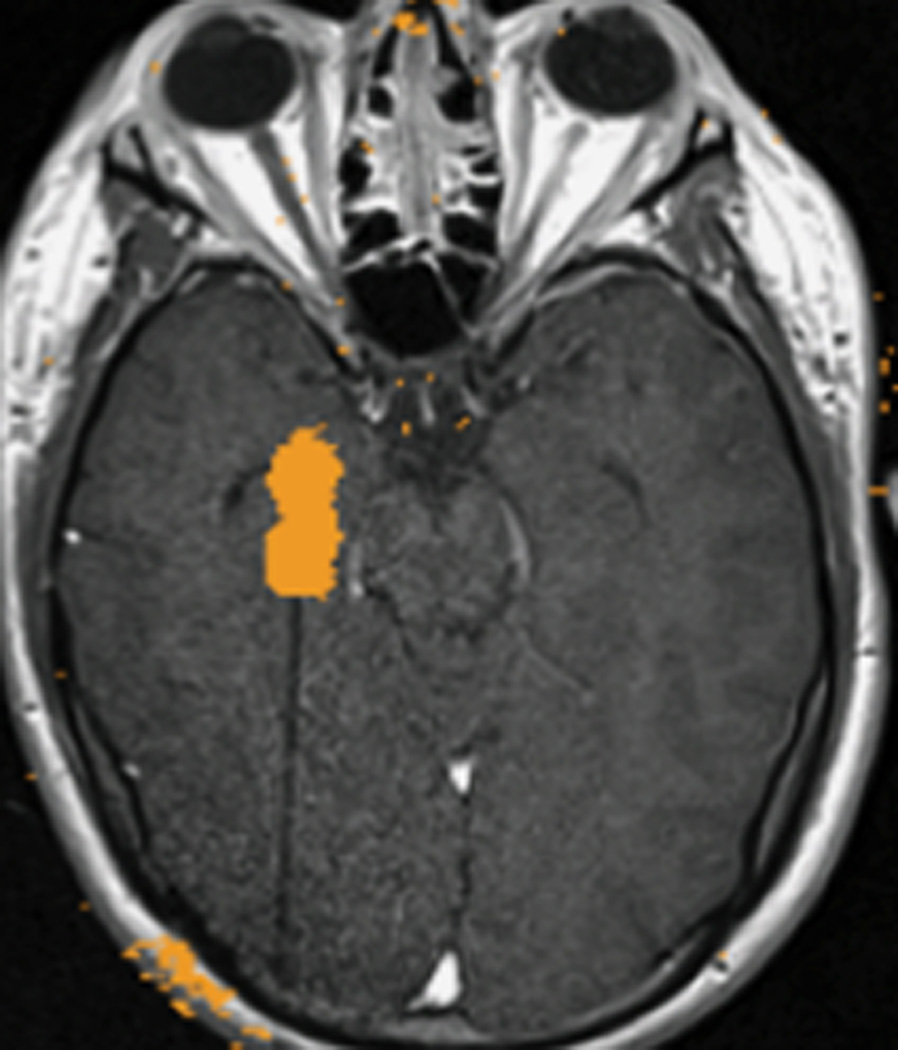
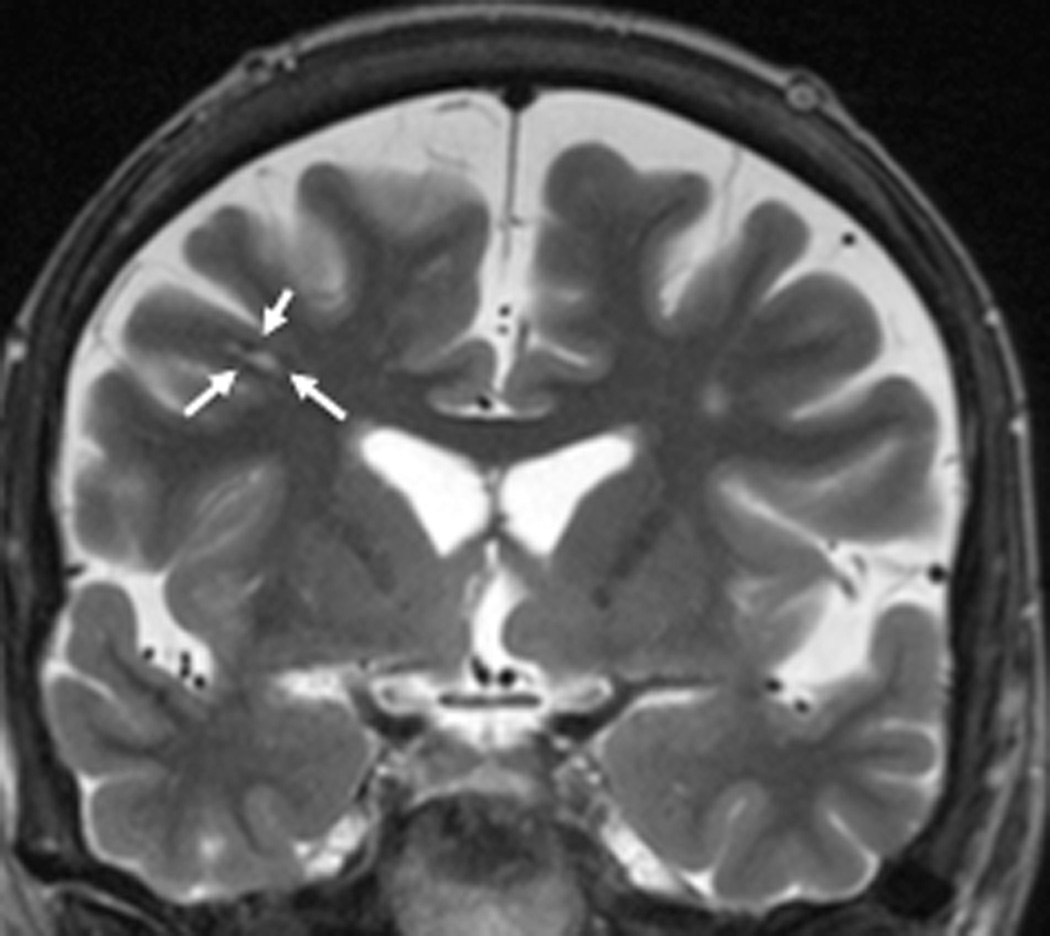
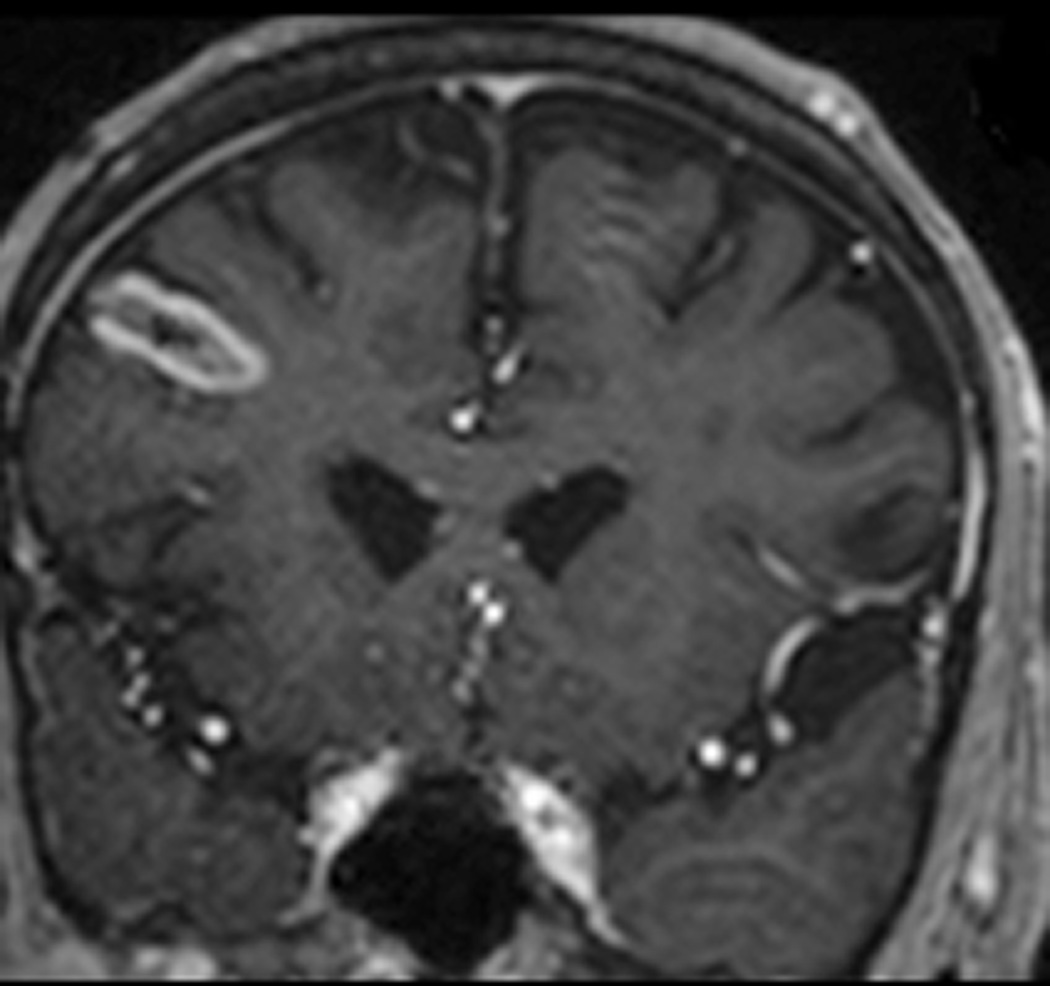
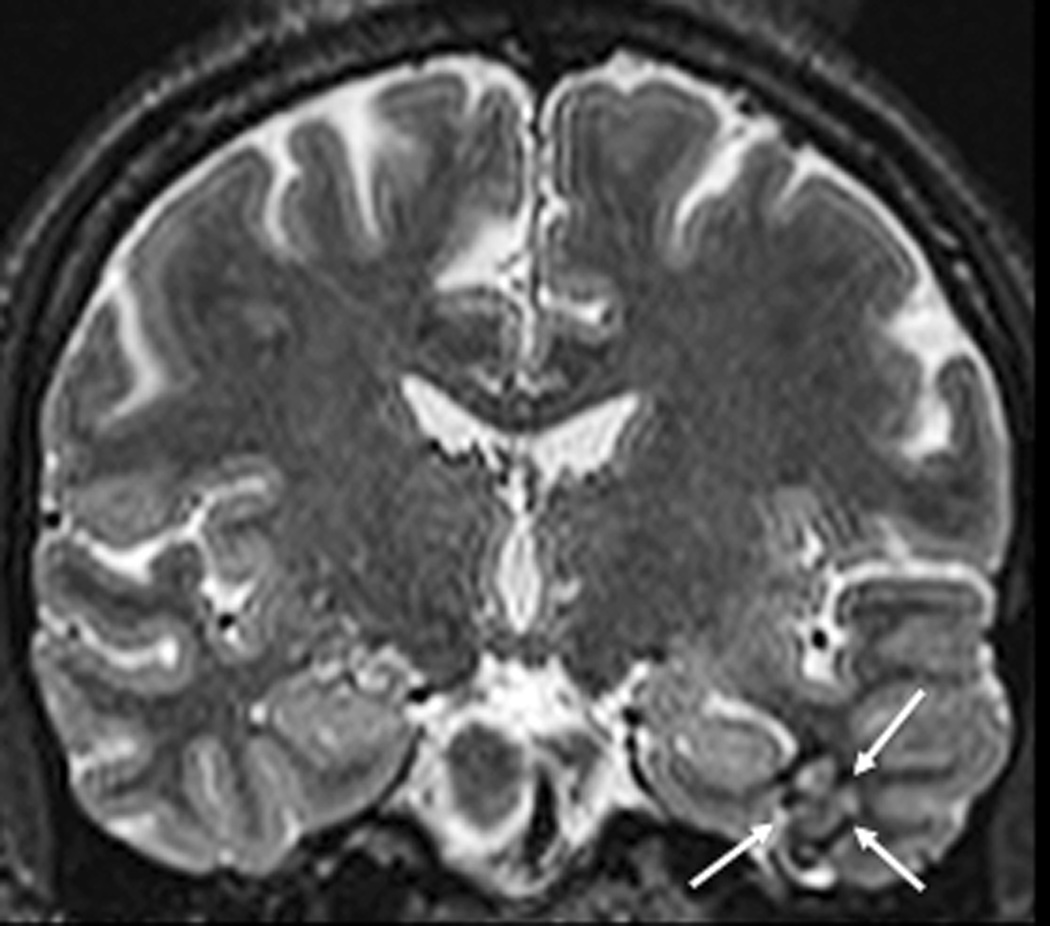
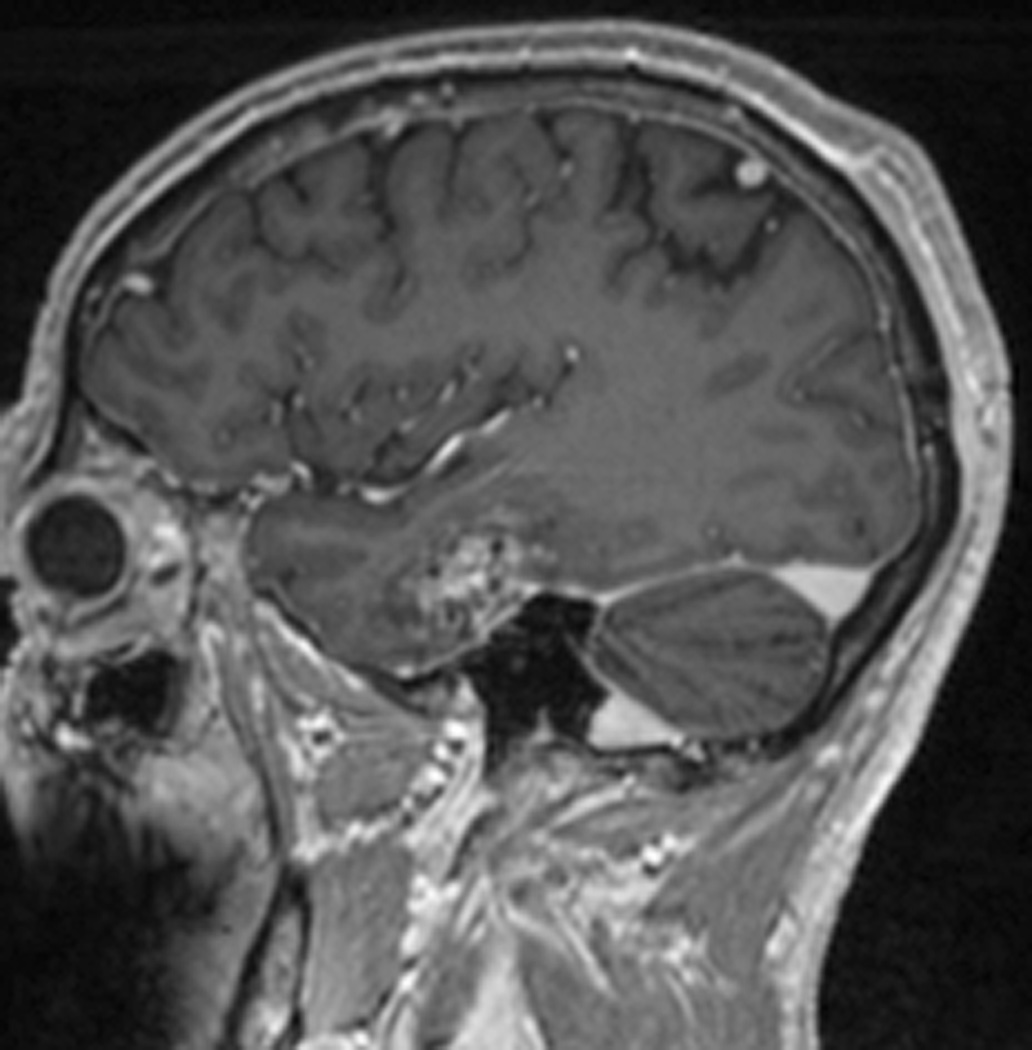
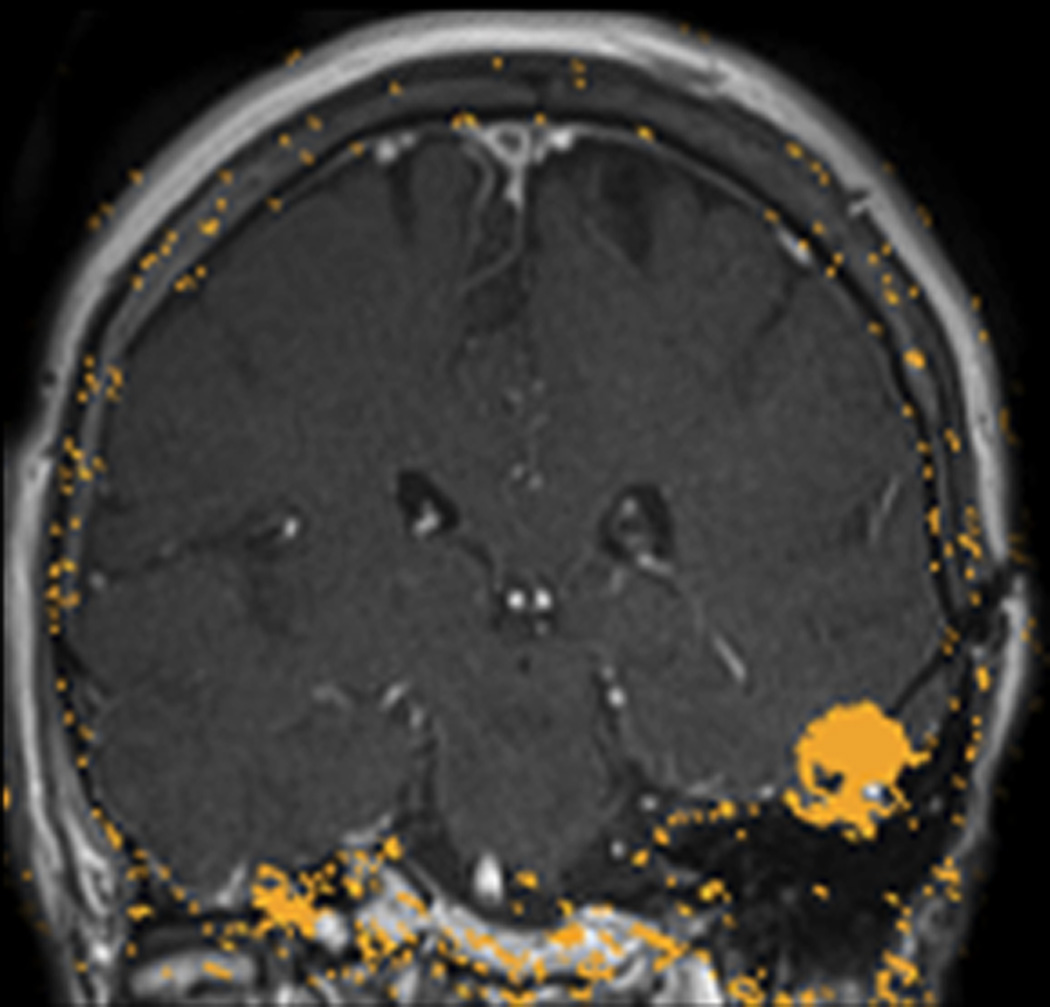
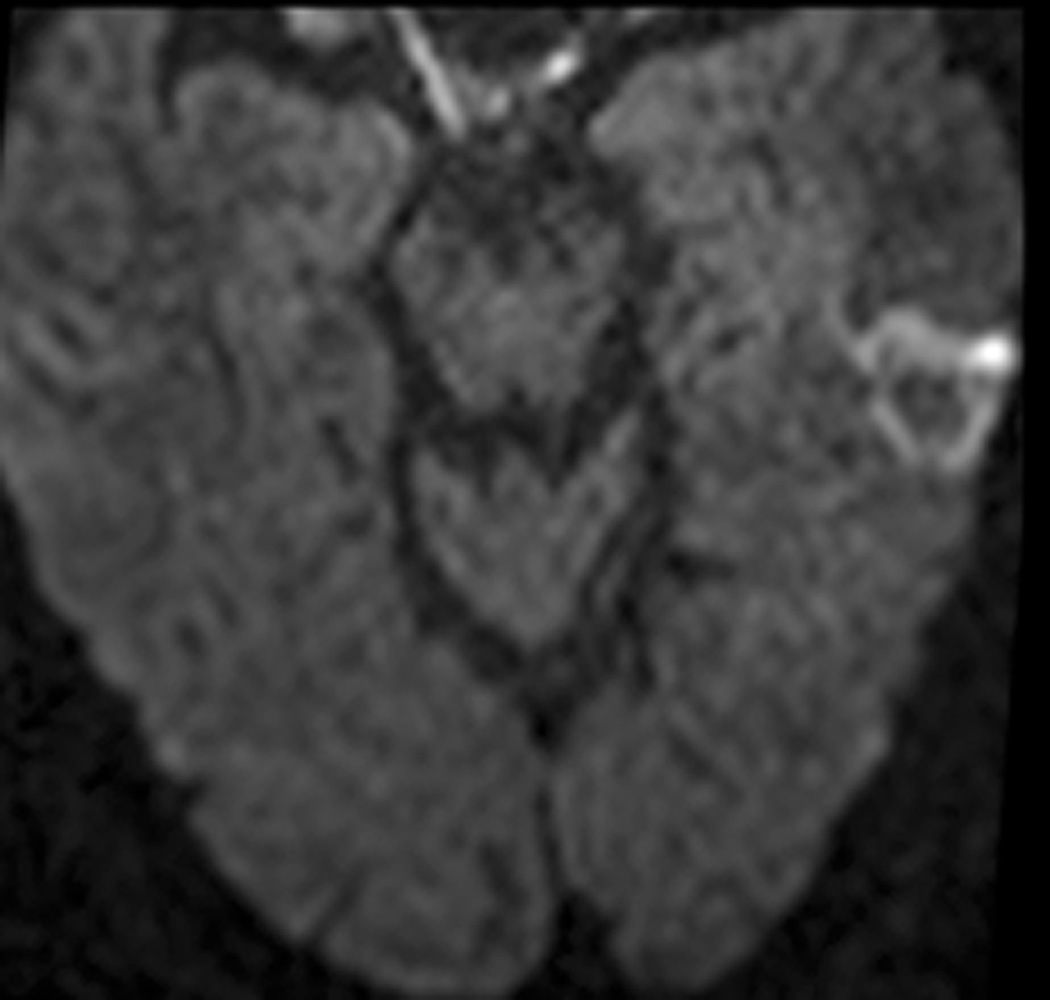
Methods: Five patients with medically refractory epilepsy undergoing standard presurgical evaluation were found to have corresponding lesions fulfilling imaging characteristics of CCM and were prospectively enrolled. Each underwent stereotactic placement of a saline-cooled cannula containing an optical fiber to deliver 980-nm diode laser energy via twist drill craniostomy. MR anatomic imaging was used to evaluate targeting prior to ablation. MR imaging provided evaluation of targeting and near real-time feedback regarding extent of tissue thermocoagulation. Patients maintained seizure diaries, and remote imaging (6-21 months post-ablation) was obtained in all patients.
Results: Imaging revealed no evidence of acute hemorrhage following fiber placement within presumed CCM. MRT during treatment and immediate post-procedure imaging confirmed desired extent of ablation. We identified no adverse events or neurological deficits. Four of 5 (80%) patients achieved freedom from disabling seizures after SLA alone (Engel class 1 outcome), with follow-up ranging 12-28 months. Reimaging of all subjects (6-21 months) indicated lesion diminution with surrounding liquefactive necrosis, consistent with the surgical goal of extended lesionotomy.
Conclusion: Minimally invasive MRT-guided SLA of epileptogenic CCM is a potentially safe and effective alternative to open resection. Additional experience and longer follow-up are needed.
Keywords: Epilepsy; cavernous malformation; laser therapy; magnetic resonance imaging; minimally invasive surgical procedures; stereotactic techniques; thermometry.
Conflict of interest statement
The terms of this arrangement have been reviewed and approved by Emory University in accordance with its conflict of interest policies.
Figures




























References
-
- Raychaudhuri R, Batjer HH, Awad IA. Intracranial cavernous angioma: a practical review of clinical and biological aspects. Surgical neurology. 2005 Apr;63(4):319–328. discussion 328. - PubMed
-
- Baumann CR, Schuknecht B, Lo Russo G, et al. Seizure outcome after resection of cavernous malformations is better when surrounding hemosiderin-stained brain also is removed. Epilepsia. 2006 Mar;47(3):563–566. - PubMed
-
- Brelie Cvd, von Lehe M, Raabe A, et al. Surgical Resection Can Be Successful in a Large Fraction of Patients With Drug-Resistant Epilepsy Associated With Multiple Cerebral Cavernous Malformations. Neurosurgery. 2014;74(2):147–153. - PubMed
-
- Kim W, Stramotas S, Choy W, Dye J, Nagasawa D, Yang I. Prognostic factors for post-operative seizure outcomes after cavernous malformation treatment. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2011 Jul;18(7):877–880. - PubMed
-
- Kim M, Rowed DW, Cheung G, Ang LC. Cavernous malformation presenting as an extra-axial cerebellopontine angle mass: case report. Neurosurgery. 1997 Jan;40(1):187–190. - PubMed
